INTRODUCTION
Vertebral mycoses are subtypes of vertebral osteomyelitis (VO) that represent rare and severe life-threatening conditions, requiring long-term pharmacological therapy and often surgical treatments [1,2]. Aspergillus species are ubiquitous fungi. They are commonly found in the upper human respiratory tract, and rarely determine infectious diseases in immunocompetent patients. On the other hand, these infections may be associated with high mortality rates in immunocompromised patients [1]. Vertebral aspergillosis (VA) represents the most frequent extrapulmonary aspergillosis localization [3]. VA may determine osteolysis, intervertebral disc involvement, and epidural space collections, resulting in painful conditions neurological symptoms, and deformities. Early diagnosis, by blood cultures or direct sampling, and a proper medical therapy represent the key points in VA management [3,4]. Few cases of VA were reported, and a consensus on diagnostic criteria and the most effective medical treatment are still missing. Since fungal infections may be undiagnosed using standard laboratory tests and cultures, specific radiological or clinical signs suspicious for Aspergillus osteomyelitis would be helpful.
We present a case of spontaneous VA, sustained by Aspergillus fumigatus, and report the results of a systematic review of the international medical literature for epidemiology, clinical-radiological aspects, treatment protocols, and outcomes of Aspergillus-mediated VO.
MATERIALS AND METHODS
1. Study Design
The present investigation consists of a case report and a systematic review of the literature conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.
2. Eligibility Criteria
English written papers on spine infections sustained by Aspergillus, reporting demographical and clinical data, diagnostic work-flow, treatment protocol, complications, and prognosis were considered for eligibility. Exclusion criteria were: surgical technique reports, expert opinions, studies on animals, unpublished reports, cadaver or in vitro investigations, book chapters, abstracts from scientific meetings, articles describing postsurgical or postinjection VA.
3. Information Sources and Search Strategy
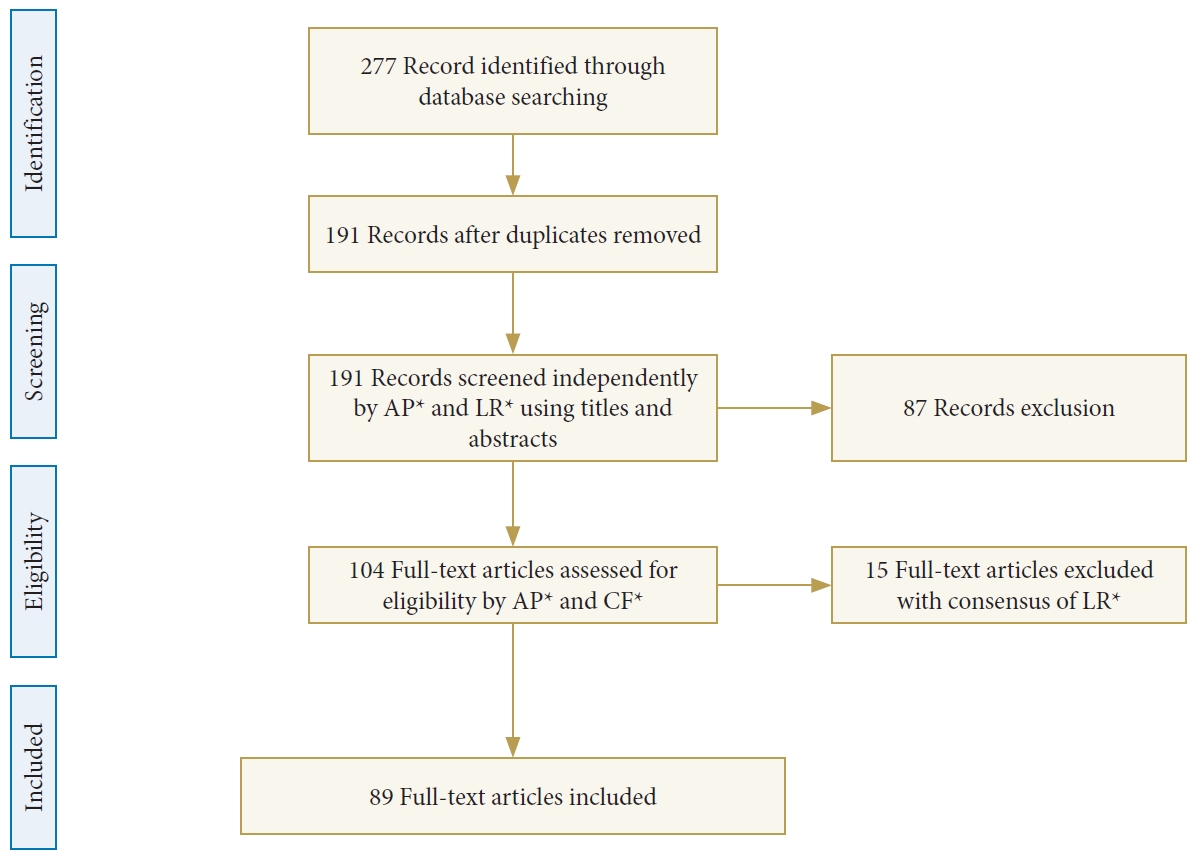
The systematic review of the literature was conducted on 4 different online medical databases (Cochrane library, MEDLINE, PubMed, Scopus), using as search-terms “Aspergillus,” “vertebral osteomyelitis,” “spondylodiscitis,” “spine infection” [MeSH], combined with the Boolean operators “AND,” “OR,” and “NOT.” The search was reiterated until 20th March 2020. The search strategy is summarized in Fig. 1.
4. Data Collection Process and Study Selections
Abstracts and full-texts were independently screened by 2 authors (AP and LR), and any discordance was solved by consensus with a third senior author (LP). The full-texts of eligible papers and their references lists (forward search) were evaluated for inclusion.
CASE REPORT
A 76-year-old man was admitted to our Emergency Department on March 2019, reporting acute low back pain, rated as 9 on a 10-point itemized visual analogue scale (VAS), and lower extremity numbness started 2 months earlier, without fever. Patient medical background showed chronic lymphocytic leukemia (CLL) in treatment with ibrutinib, atrial fibrillation, and severe aortic stenosis; no alcohol or drugs abuse, smoking status, dental procedures, or recurrent infections were reported. The physical examination showed upper lumbar localized pain, worsened by the axial load and thoracic flexion; bilateral lower limbs paresthesia without motor deficits was observed.
Laboratory blood tests showed increased values of C-reactive protein (CRP: 66.2 mg/L; normal value, < 5), erythrocyte sedimentation rate (ESR: 45 mm/hr; normal value, <30), white blood cells (WBC) count (8,580 elements per mm3), and negative blood cultures for bacterial. QuantiFERON-Tb Gold and human immunodeficiency virus serology were negative.
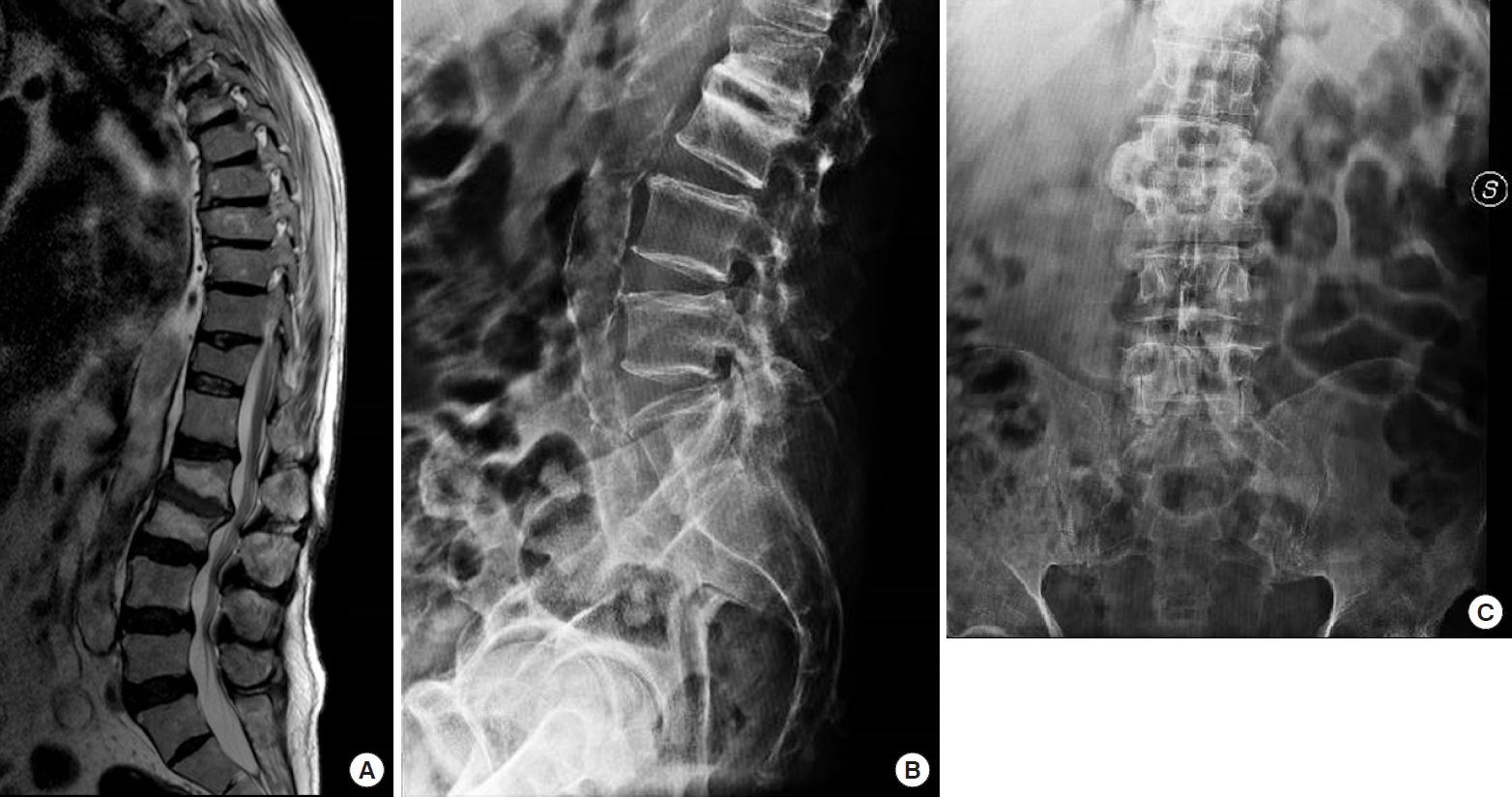
Lumbar spine computed tomography (CT) scan and magnetic resonance imaging (MRI) revealed a spondylodiscitis on L2–3 disc (Fig. 2). Imaging of the chest, skull, and paranasal sinuses did not show any significant finding. A CT-guided needle biopsy was performed on L2–3 and the collected samples were cultured for bacterial and fungal species. The following media were used for mycotic culturing: Candida BCG agar (Meus, Italy) and Saboraud Dextrose Agar+CAF tube (Meus). Filamentous mycelium was found on both media was observed within 72 hours. Matrix-assisted laser desorption/ionization-time of flight mass spectrometry technology, directly from colonies grown on culture plates [5], identified A. fumigatus. Nonculture-based assays, that the patient had for CLL, showed low levels of 1,3-beta-D-glucan (BDG Fungitell assay) on 3 consecutive serum samples (186, 253, and 145 pg/mL), respectively 12, 10, and 6 weeks before the diagnosis. At the time of the diagnosis serum, 1,3-beta-D-glucan value was negative (< 80 pg/mL). The galactomannan serum Index (GM Platelia assay) was also negative. Intravenous administration of liposomal amphotericin B was promptly started, and the patient was immobilized in a rigid fiberglass brace.
After 30 days of medical treatment and immobilization, CRP and ESR values and the WBC count reported a decreasing trend, and back pain and lower extremities numbness improved as well; therefore, oral voriconazole and a rigid bracing were prescribed, then the patient was discharged. At the 3 months follow-up visit, the patient reported minimal low back pain (VAS 2); the MRI showed an improvement of the radiological scenario the local inflammatory pattern. After 6 months, the MRI and the x-rays showed a further improvement, with no longer signs of active inflammatory process or neurological compression and no signs of segmental or spinal deformity (Fig. 3). Accordingly, voriconazole oral therapy was stopped. No antibiotic therapy-side effects were recorded. The patient was pain free and able to walk for up to 400 m, hence he was advised to progressively weaning the brace. The patient signed a specific consensus for scientific purposes, according to the institutional guidelines.
RESULTS
1. Study Selection and Characteristics
After duplication removal 191 papers were considered for eligibility in the present systematic review. Eighty-seven papers were excluded for the following reason according to the exclusion criteria: non-English written papers (27), cases of Aspergillosis with no spinal involvement (44), non-Aspergillosis mediated spinal infections (16). Therefore, 104 full-text papers were evaluated. Fifteen cases of postsurgical or postinjection VA were also reported and excluded according to our inclusion criteria. Finally, 89 papers reporting 112 cases, including our case report, of spontaneous VA were included in the present review [3,6-94]. The mean age of included patients was 41.4 ±18.9 years, 16 (14.4%) were pediatric (< 18 years), and the male/female ratio was 2.6:1. Demographic and clinical data are summarized in Table 1.
2. Localization, Symptoms, and Risk Factors
VA seems to be slightly prevalent in the thoracic spine (46.8%), followed by the lumbar (42.3%) and cervical (10.9%) segments. Single localizations were found in 76 patients (67.6%), while multiple localization in 36 (32.4%), comprising 11 cases (9.9%) of skipped locations. Abscesses were reported in 79 cases (70.3%): epidural abscess in 35 (31.2%), paravertebral in 34 (30.3%), and both paravertebral and epidural in 10 (8.9%). The presenting symptoms were: back pain (57%) in 64 patients, lower extremity weakness in 35 (31.2%), and fever in 14 (12.5%). The authors reported as risk factors were: pulmonary aspergillosis (22.5%), hematological malignancies (17.1%), immunosuppressive therapy after organ transplantation (13.5%), and chronic granulomatosis disease (9%) [95].
3. Diagnosis and Etiology
The diagnostic sample was obtained by open biopsy in 78 cases (79.2%), needle biopsy in 32 (28.8%), blood culture confirmed by open biopsy in 1 (0.9%), and postmortem investigations in 1 (0.9%).
The etiological diagnosis was made by culturing samples in 61 cases (54.9%), histological examination confirmed by cultures in 36 (32.4%), histological examination only in 11 (9.9%), polymerase chain reaction (PCR) in 3 (2.7%), and cytological examination in 1 (0.9%). Isolated species was A. fumigatus in 68 cases (61.2%), Aspergillus flavus in 14 (12.6%), Aspergillus terreus in 4 (3.6%), Aspergillus nidulans in 2 (1.8%), Aspergillus niger in 1 (0.9%), and Aspergillus udagawae in 1 (0.9%). In 22 cases (20.8%), Aspergillus specie was not specified.
4. Treatment Protocols
Medical treatment alone was administered in 23 patients (20.7%), while in 89 (80.1%) adjuvant surgery was reported: posterior or anterior decompression and local debridement was performed in 49 patients (44.1%), anterior decompression and fusion with autologous bone graft in 20 (18%), decompression and circumferential fusion in 13 (11.7%), and posterior decompression and fusion in 7 (6.3%).
Medical treatments consisted in (1) single drug in 54 cases (48.6%): amphotericin B in 31 patients (27.9%), voriconazole in 12 (10.8%), itraconazole in 10 (9%), and fluconazole in 1 (0.9%); (2) combination of 2 or more drugs in 50 patients (45%): amphotericin B+flucytosine in 10 cases (9%), amphotericin B+itraconazole in 11 (9.9%), amphotericin B+voriconazole in 4 (3.6%), amphotericin B+flucytosine+itraconazole in 4 (3.6%), and amphotericin B+fluconazole in 2 (1.8%).
The mean duration of therapy was 140±247.9 days.
5. Clinical Outcomes and Complications
Seventy-three patients (65.7%) completely recovered at the last follow-up evaluation; radiological signs of chronic infection were reported in 7 patients (6.3%), whereas 32 patients (28.8%) died during the follow-up. The complication rate was as high as 36%. Neurological sequelae were reported in 10 cases (9%), recurrence of the infection in 9 (8.1%), spine deformity in 8 (7.2%), sepsis in 6 (5.4%), and respiratory failure in 5 (4.5%). Regarding medical therapy-associated complications, liver and renal dysfunction occurred in 10 (9%) and 6 cases (5.4%), respectively.
DISCUSSION
1. Etiology and Pathogenesis
Aspergillosis represents a rare disease, and its incidence is estimated of 12 cases per year/1,000,000 people [60]; on the other hand, it has been frequently reported in immunodeficient patients [1]. VA is the most common Aspergillus-mediated osteomyelitis [3], and 20 different species of Aspergillus can cause infections in humans [96]. The most involved species is A. fumigatus [96], whereas A. flavus, A. niger, and A. nidulans are rarely isolated.
Three different pathogenetic mechanisms have been proposed: direct invasion by contiguous pulmonary foci, hematogenous diffusion, and iatrogenic or traumatic inoculation. Pulmonary aspergillosis represents the most relevant risk factor for VA, reported in 22% of the cases [95].
2. Diagnosis
Diagnosis of spondylodiscitis sustained by Aspergillus is currently based on cultures and histological examination [79,96]. The role of serum galactomannan in VA is still debated [79], whereas the PCR on bone samples has not been validated yet, although it could be useful in the case of nondiagnostic culture and histology. The clinical presentation does not recognize any pathognomonic symptom or sign, as well as in pyogenic spondylodiscitis [97,98]. Back pain and neurological deficits are commonly reported by patients at the time of hospitalization, affecting the chances for a correct diagnosis [99]. Spinal cord and/or radicular compression can be determined by VO, epidural abscess, Aspergillus granuloma, vertebral fractures, and postinfectious deformities [60]. Gadolinium-enhanced MRI sequences may help in identifying infectious collections, abscesses, and granulomas [100]; therefore, neuroimaging should be carefully evaluated by experienced radiologists.
3. Treatment Work-Flow
A targeted medical antifungal therapy may result in increased chances for better clinical outcomes in VA, thus the isolation of the involved pathogen is strongly recommended. Percutaneous sampling under radiological guidance may represent a useful alternative to open biopsy [2]. However, worsening neurological symptoms and/or poor response to medical therapies may lead to surgical decompression [2]. Surgery may be useful to achieve a solid fusion and deformity correction in case of spinal instability or vertebral collapse and obtain a microbiological sample to reach the diagnosis in case of negative needle biopsy [100-102].
Medical treatment should be customized for each patient. Vertebral instability, neurological compression, and local progression in course of the antifungal therapy should be carefully considered as criteria for surgery [79].
4. Antifungal Agents
Up to date, either amphotericin or voriconazole is the recommended antifungal agents for the treatment of Aspergillus osteomyelitis according to The Infectious Diseases Society of America guidelines [103]. Voriconazole has been reported as the first choice, because of its high bioavailability and tissue penetration, even though its pharmacological interactions, the necessity of therapeutic drug monitoring (TDM), liver toxicity, and photosensitivity may influence its role in prolonged therapies. Liposomal amphotericin B is an alternative to be considered, although it is available only for intravenous usage, and has been associated with nephrotoxicity [103]. However, the British Infection Society recommends the use of liposomal amphotericin B in combination with flucytosine as the first choice for the treatment of Aspergillus osteomyelitis [1]. The use of itraconazole should be reserved for the treatment of stable patients. In fact, it can be effective in osteoarticular aspergillosis reporting a toxicity profile similar to voriconazole, and a lower bioavailability. Isavuconazole has a higher bioavailability and safety profile compared with voriconazole, and does not require TDM; however, it has been anecdotally used in VA. Posaconazole was proposed in 2 case reports only [104,105].
5. Therapy Duration
There is no consensus on the optimal antifungal therapy duration for Aspergillus osteomyelitis. Infectious Diseases Society of America guidelines for the treatment of Aspergillus infections suggested a minimum of 8 weeks, although longer administrations (> 6 months) are often needed [103]. Furthermore, these recommendations do not consider the role of surgery and its influence on medical treatment duration.
There some limitations we need to report for proper data interpretation. All the included studies are case report or case series, reporting a low level of evidence (IV-V). The publication time range of the included papers is longer than 50 years. Data have been reported in a nonhomogeneous way among the included papers, thus not allowing the authors to conduct any data pooling for statistical analysis.
In conclusion, VA is a rare condition, although its real incidence could have been underestimated due to diagnostic limitations. Fungal species should be routinely investigated in culture-negative spondylodiscitis, especially in immunocompromised patients. Since VA has a poor prognosis, an early diagnosis for targeted medical therapy should be always pursued. This systematic review summarized the state of the art on VA, retrieving data on clinical features, diagnostic criteria, and current limitations, treatment alternatives, and their outcomes, along with future perspectives for the clinical management. Further clinical studies are needed to better investigate this challenging topic.