INTRODUCTION
Posterolateral lumbar fusion (PLF) is performed to correct adult spinal deformity (ASD) [1]. Autologous bone grafts for PLF are usually harvested from the iliac crest, requiring additional surgery; moreover, it may not yield sufficient bone. It can also be associated with donor site complications (hematoma, fracture, wound healing problems, persistent pain, pelvic deformity, and neurovascular injuries) [2-5]. Many ASD cases require multilevel fusion, requiring more bone grafts than typical single-level fusion. Thus, multilevel fusion decreases the union rate and increases surgical blood loss, operative time, length of hospital stay, and recovery time [6].
Various materials have been explored as autogenous bone substitutes. However, noncalcium phosphate-based bone substitutes demonstrate poor mechanical properties, low biocompatibility, and poor tissue adhesion. Therefore, calcium phosphate-based ceramics, such as hydroxyapatite (HA), have been developed to address these issues. HA is a naturally-occurring form of calcium phosphate and the most abundant inorganic constituent of human bones [7]. Unlike allografts, HA shows no risk of virus transmission. Moreover, it is nonallergenic with excellent osseointegration. Therefore, HA is preferred as a bone graft or extender in orthopedics [8-11].
Bone morphogenetic proteins (BMPs) have been considered for bone graft enhancement. Among the various BMPs, factors with osteogenic activity are limited [12]. Recombinant human BMP-2 (rhBMP-2) is commercially available and approved by the U.S. Food and Drug Administration for anterior lumbar interbody fusion (ALIF) [13]. Treatment with rhBMP-2 results in a higher union rate than autologous bone and significantly improves several clinical parameters in a single-level fusion through ALIF and PLF [14-16]. Mulconrey et al. [17] demonstrated rhBMP-2 efficacy in multilevel fusion in 98 patients with ASD. Application of rhBMP-2 at an average of 2.6 levels per patient resulted in a 95% union rate. However, these studies have not identified any interpatient factors with statistically significant effects on the bone union. Therefore, this investigator-initiated exploratory study on multilevel fusion compared the outcomes of the combined use of rhBMP-2 and HA to HA alone in the same patients to exclude interpatient factors.
MATERIALS AND METHODS
1. Study Design
This study was a investigator-initiated, prospective, single-center, randomized, controlled, exploratory clinical trial. Patients were enrolled with institutional review board approval between October 2016 and December 2019. This study was registered with the Clinical Research Information Service (CRIS No. KCT-0006545) and conducted according to the principles of the Declaration of Helsinki and the guidelines of Good Clinical Practice.
Patients who visited to the clinic and met the following inclusion criteria were consecutively enrolled: (1) age, 19–80 years, (2) pain associated with ASD at 3–5 segments between L1 and S1 necessitating intertransverse process lateral fusion, (3) voluntary participation in this clinical trial with written consent. The exclusion criteria were as follows: (1) participation in another clinical trial within 1 month before enrollment, (2) history of fusion surgery on the same site, (3) osteoporosis; average T-score ≤ -3.0 at lumbar, (4) immunosuppression or autoimmune disease, (5) rhBMP-2 hypersensitivity, (6) history of malignant tumors, (7) fractures, acute infections, hemorrhagic diseases, active systemic infections, osteodystrophy, or infections at the surgical site, (8) serious diseases that could affect surgery, (9) use of contraindicated concomitant drugs, (10) alcohol or drug addiction, or mental illness, (11) pregnancy, lactation. Detailed criteria for ASD are scoliosis Cobb angle of 20° or more, sagittal vertical axis of 5 cm or more, pelvic tilt of 25° or more, and/or pelvic incidence–lumbar lordosis of 10° or more. All patients enrolled in this study received the same posterior column osteotomy, and none underwent 3-column osteotomy that would have been a confounder to the study. Since this is an investigator-initiated exploratory trial, the sample size was not statistically calculated. In addition, the clinically significant effect sizes, limits, and standard deviations required to calculate the number of subjects could not be obtained due to the absence of adequate previous studies. The number of subjects was determined based on clinical experience (the number of patients visiting the hospital, the enrollment rate, etc.) and the dropout rate of 20%. Eligible subjects were assigned numbers according to pregenerated randomization of the order of participation. A block randomization was conducted through a web-based simple randomization service (https://www.sealedenvelope.com/simple-randomiser/v1/lists) provided by Sealed Envelope. Control (HA) or test sites (rhBMP-2+HA) were randomly assigned to the left or right side of one patient's transverse processes in a 1:1 ratio. The surgeon was blinded until the day of surgery and was unable to preidentify the randomization code for the patient. Patients received follow-ups at 1, 3, 6, and 12 months after surgery with physical examination and static radiography at every follow-up visit, dynamic radiography at 3, 6, and 12 months after surgery, and computed tomography (CT) scans at 6 and 12 months following surgery. For clinical outcomes, we evaluated visual analogue scale (VAS) and Oswestry Disability Index (ODI) scores for back and leg pain at baseline and at 6 and 12 months after surgery. 36-item Short Form Health Survey (SF-36) and Scoliosis Research Society-22 (SRS-22) questionnaires were administered at baseline and 12 months after surgery. Samples for rhBMP-2 antibody testing were collected and analyzed at baseline and at 3 and 12 months after surgery.
2. Intervention
After general anesthesia, we used a midline skin incision and a posterior approach [18,19] to expose the origin of the transverse processes on both sides, with bilateral retraction. The affected nerve root was decompressed by laminectomy. Pedicle screws were inserted into the vertebral body with an appropriate medical angulation. The anterior cortical bone of the vertebra was fixed to sufficient depth without damage using a rod. The lateral surface of the vertebral joint, the recess at the origin of the transverse process, and the bone surface of the transverse process were removed and irrigated with saline. Bone grafts were placed on the assigned side according to randomization results. Instrumentation was performed at all fused segments. The test site (rhBMP-2+HA) received 3.0 g of a porous HA carrier (Bongros-HA, CG Bio Co., Ltd., Seoul, Korea) adsorbed with 3.0 mg of E. coli-derived rhBMP-2 (Novosis, CG Bio Co., Ltd., Seoul, Korea) per level for posterolateral bone fusion. The average amount of rhBMP-2 applied per patient was 12.78 ± 2.71 mg (9–15 mg rhBMP-2 for 3–5 level fusion). The dose setting of 3.0 mg of rhBMP-2 per level was based on previous studies [16]. For the control site (HA), 3.0 g of HA carrier, loaded with saline, was mixed with 2.5 g of HA carrier only and transplanted.
3. Evaluation
The primary efficacy endpoint was the CT-based union rate at 12 months, and the secondary efficacy endpoint was the CT-based union rate at 6 months. The union was judged as grade I–IV according to the bone bridging pattern on the CT scan as follows [20]: grade I, complete fusion; grade II, partial fusion; grade III, unipolar pseudarthrosis; grade IV, bipolar pseudarthrosis. Grades I and II were considered “bone union.” Two spinal neurosurgeons who did not participate in this study evaluated the results as independent evaluators. Where there were conflicting opinions between the 2 evaluators, the result was nonunion. In this study, “union” was judged only when all segments were fused and “nonunion” when even one segment was not fused. The evaluation was subject and operator-blinded, and the sites for assessment (test and control site) were also blinded to minimize bias. Changes in VAS, ODI, SF-36, and SRS-22 scores were considered secondary endpoints. We counted subjects with adverse events (AEs) during the clinical trial to evaluate safety. The proportion of subjects experiencing AEs was analyzed separately for treatment-emergent AEs (TEAEs) and adverse device events (ADEs), with an additional analysis based on severity.
4. rhBMP-2 Antibody Analysis
We modified the study plan for analyzing increased rhBMP-2 antibodies during the clinical trial. An enzyme-linked immunosorbent assay-based rhBMP-2 antibody test was performed on 11 patients enrolled after plan modification, and serum samples were collected at baseline and at 3 and 12 months after surgery. A difference in absorbance before and after surgery of more than 3 times the standard deviation of baseline samples was considered positive for antibody elevation (following antibody test guidelines).
5. Statistical Analysis
Demographic data were descriptively analyzed. The union rate was presented as a number (n) and a ratio (%), and the difference between the groups was analyzed using McNemar test. Interobserver reliability for the reading of fusion status on CT scans was evaluated using Cohen kappa (Definition [21]: 0.01‒0.20 slight agreement, 0.21‒0.40 fair agreement, 0.41‒0.60 moderate agreement, 0.61‒0.80 substantial agreement, 0.81‒1.00 almost perfect or perfect agreement). Changes in VAS, ODI, SF-36, and SRS-22 scores from baseline were analyzed using the paired t-test or Wilcoxon signed-rank test. Two-sample t-test or Mann-Whitney U-test was used to compare demographic factors in union and non-union cases. Statistical analysis was performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The threshold for statistical significance was set at p< 0.05.
RESULTS
1. Patients
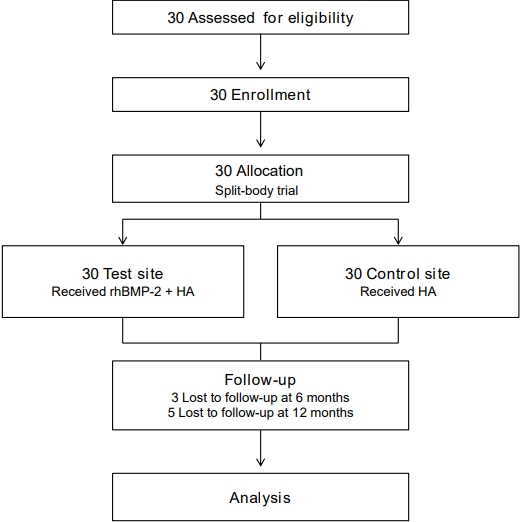
Thirty subjects were enrolled after screening. We included 27 subjects for analysis at 6 months and 25 subjects at 12 months. The number of subjects enrolled, assigned, lost at follow-up, and analyzed are summarized in the flow diagram (Fig. 1). Data on patient baseline characteristics and operated segments are presented in Table 1.
2. Union Rate
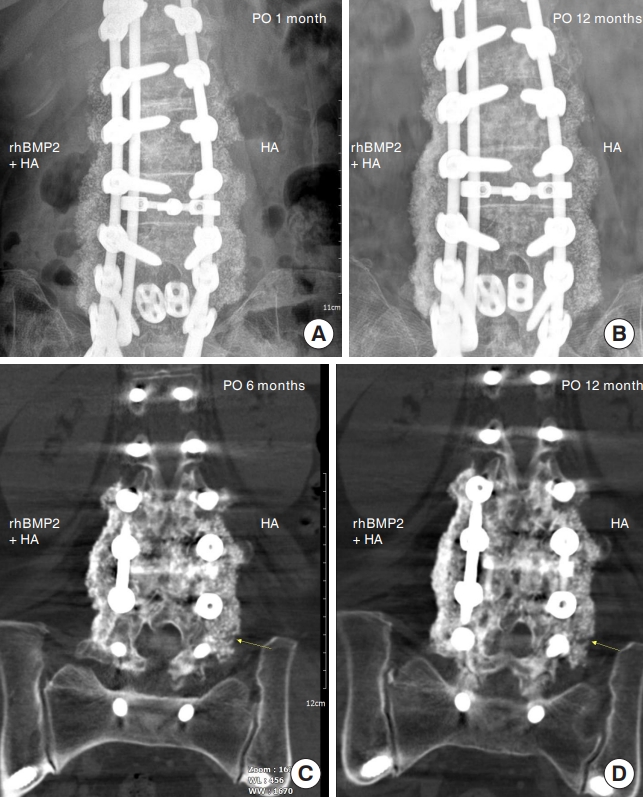
We evaluated the union rates separately for control and test sites (Table 2). At 6 months, the union rate was 100% (27 of 27) at the test site and 77.8% (21 of 27) at the control site, indicating a statistically significantly higher union rate at the test site (p= 0.014). At 12 months, the union rate was 100% (25 of 25) at the test site and 88.0% (22 of 25) at the control site (p= 0.083). Based on Cohen kappa (0.86), interobserver reliability between evaluators (98.1%) for fusion evaluation indicated almost perfect agreement. The union rate per segment was subanalyzed (Table 3). In the subanalysis, a total of 115 segments (in 27 patients) were included at 6 months and 109 segments (in 25 patients) at 12 months. The union rate at the control site was 93.9% (108 of 115) at 6 months and 96.3% (105 of 109) at 12 months. At 6 months, 6 of 7 nonunion segments were L5–S1, and one was L3–4. At 12 months, 3 of 4 nonunion segments were L5–S1 and one L3–4. In the test group, the union rates at 6 and 12 months were both 100%, and the differences between the groups were significant at both time points (p< 0.001). Fusion characteristics on CT scans were slightly different between the 2 groups. Although both sites showed fusion mass, continuity of the fused mass was more prominent and uniformly observed at the test site than at the control site (Fig. 2).
3. Clinical Outcomes
ODI and VAS scores for back and leg pain significantly decreased compared to baseline at all time points (all p < 0.01) (Table 4). The Physical Component Summary and Mental Component Summary scores in the SF-36 questionnaire (to evaluate the quality of daily life) had significantly improved 12 months after surgery compared to baseline (p < 0.001) (Table 5). The SRS-22 score significantly improved compared to baseline values (p< 0.001) (Table 5).
4. Safety
We analyzed safety in 30 enrolled subjects. Eleven subjects had TEAEs (36.67%, 23 cases). Among TEAEs, fluid collection at the surgical site developed in 2 patients, but symptoms (buttock pain) improved after percutaneous catheter drainage, and bacterial cultures were negative.
Three patients (10.0%) had 4 serious TEAEs, 1 mild (adjacent disc herniation at T8‒9 at 9‒12 months), and 3 moderate (acute kidney injury between baseline and 1 month, thoracic vertebral compression fracture at T11 at 1‒3 months, gait disturbance after 12 months). Most serious TEAEs (3 patients) resolved with conservative drug treatment and rehabilitation. However, one patient with a fracture recovered after 8 weeks of fusion extension surgery. No subject developed ADEs or serious ADEs. Laboratory and electrocardiogram tests revealed no abnormal findings.
We analyzed the antibody response according to the high-dose rhBMP-2. One patient was temporarily positive at 3 months but negative at 12 months. This patient achieved radiographic union at both control and test sites at all time points, with no rhBMP2-related complications.
DISCUSSION
This study had a split-body trial design with a control or test site assigned to the left/right side of the transverse process of one subject. An average of 4.26 segments were fused. The union rate at the test site was 100% at 6 and 12 months. Despite using multilevel fusion, our results were similar to previously reported union rates achieved with rhBMP-2 with single-level fusion. Cho et al. [16] applied 3.0 mg of rhBMP-2 along with an HA carrier to a single level PLF. The union rate achieved in the rhBMP-2+HA group at 3 and 6 months was 100%, superior to that of the ICBG group (3 months, 90.2%; 6 months, 94.1%). Therefore, the present study demonstrated that 3.0 mg of rhBMP-2 per level was sufficient to achieve bone fusion, even at multiple fusion levels (3–5 levels).
In the HA group, we applied a high-purity synthetic HA ceramic with a structure in which 300‒500 μm pores are 3-dimensionally interconnected by mimicking human cancellous bone. HA is a low-biodegradable osteoconductive material that can serve as a long-term carrier due to high rhBMP-2 affinity. Because HA effectively adsorbs rhBMP-2 to the surface due to its high affinity and porosity, it can slowly and continuously release rhBMP-2 through adjacent bodily fluid streams [22-24]. This study showed a 77.8% union rate for the HA group at 6 months and 88.0% at 12 months, higher than the union rates achieved in previous PLF studies on a single level [25]. Nam and Yi [25] applied HA or demineralized bone matrix (DBM) as a bone graft extender for PLF, but the union rate at 12 months in the HA group was 58%, not significantly different from the 73% achieved in the DBM group. Our study used only the HA carrier at the control site for multilevel fusion. The high union rate achieved at the control site could be due to earlier fusion at the contralateral test site that received rhBMP-2 with HA. Early union of the test site would have a positive effect on the union rate by providing stability to the control site. Subanalysis of the union rate per segment showed that the HA group exhibited a 93.9% (108 of 115) union rate at 6 months and 96.3% (105 of 109) at 12 months. There were differences between nonunion and union cases in female ratio, BMD, smoking, drinking, number of fusion levels, and fusion sites, but only smoking showed a statistically significant difference (p= 0.001). Smoking may be a major confounder of spinal fusion. The demographic factors of the nonunion case were compared with that of the union case (Table 6). As a result of analyzing the union rate at the control site excluding 3 smokers, the union rate at 6 months was 79.2% (19 of 24), and the union rate at 12 months was 87.0% (20 of 23). The union rate per segment at 6 months was 94.2% (98 of 104), and the union rate per segment at 12 months was 96.0% (97 of 101).
The segment with the highest nonunion rate was L5–S1 (at 6 months; 85.7%; 12 months, 75.0%). The L5–S1 region exhibits a high nonunion rate due to poor sacral bone quality, complex sacral anatomy, and high biomechanical forces exerted on the lumbosacral junction [26-29]. Nevertheless, the rhBMP-2+HA group showed union at all segments and time points. Therefore, the application of rhBMP-2 with HA can increase the union rate in long-segment fusion, including the lumbosacral junction (L5–S1), where nonunions are frequent.
The rhBMP-2 is a growth factor with osteoinductive ability. Consequently, there have been concerns about side effects with high doses. This study used 3.0 mg per segment and 9–15 mg rhBMP-2 per patient. Assuming that the average weight of patients was 60 kg, the dose per patient was 0.15‒0.25 mg/kg, which was lower than the dose at which no adverse effects of rhBMP-2 were observed in rats (0.5 mg/kg) [30] and markedly lower than the lethal dose in rats (7.0 mg/kg) [31].
Some side effects associated with rhBMP-2 in the lumbar region are postoperative radiculitis, postoperative nerve root injury, ectopic bone formation, vertebral osteolysis/edema, and retrograde ejaculation [32]. However, no severe ADEs due to rhBMP-2 occurred in this study. Furthermore, this clinical trial evaluated the antibody response according to rhBMP-2 application in some subjects at 3 and 12 months. Only one subject temporarily tested positive at 3 months but negative at 12 months, a finding consistent with the results of a prospective, longitudinal cohort study. Burkus et al. [33] analyzed antibody production and clinical symptoms in patients receiving rhBMP-2 in the lumbar region. Antibody formation against rhBMP-2 peaked at 3 months and decreased to baseline at 12 months. The overall antibody elevation rate was 0.8%‒6.4%, but all were non-neutralizing antibodies [33]. These nonneutralizing antibodies generated due to an immune response to the therapeutic protein can bind to the protein without affecting its activity. Therefore, even if an antibody is present, it is important to determine whether it is a neutralizing antibody and exhibits actual clinical effects [33]. In this study, one subject with antibody formation showed bone union at both control and test sites, with no other clinical AEs.
This study had several limitations. The number of patients was too small to sufficiently detect differences in effects between groups. The follow-up period was short (1 year). Therefore, it is necessary to verify long-term clinical results with a larger cohort in the future. We applied 2 interventions simultaneously in each subject that could have mutually influenced the outcomes of each treatment group. The split-body trial has an advantage that the confounding factors between groups can be removed because the subjects of the test group are the same. However, since half of the human body is not completely independent, the difference in effects between groups may be underestimated, and systemic side effects may be masked [34]. Therefore, this study was able to directly compare the difference in effects according to BMP-2 without confounding factors between individuals, but the degree of difference may have been underestimated. In addition, safety could not be evaluated separately between groups.
In conclusion, this study demonstrated the clinical efficacy and safety of combined rhBMP-2 and HA in multilevel PLF fusion for ASD correction. Complete fusion was achieved at 6 months with 3 mg of rhBMP-2 per level for multilevel fusion (3‒5 levels) without causing antibody production that resulted in clinical symptoms.
CONCLUSION
This prospective, randomized, controlled trial investigated the efficacy and safety of the combined use of rhBMP-2 and a HA carrier in multilevel fusion in patients with ASD. The union rate for the rhBMP-2+HA group was 100% at 6 and 12 months. The union rate for the HA group was 77.8% (21 of 27) at 6 months and 88.0% (22 of 25) at 12 months. (p= 0.014 at 6 months; not significant at 12 months). In subgroup analysis per segment, 108 (93.9%) of a total of 115 segments at the control site and all segments at the test site were fused at 6 months (p< 0.001). At 12 months, 105 (96.3%) of a total of 109 segments at the control site and all segments at the test site were fused (p< 0.001). Clinical- and functional parameters (VAS, SF-36, and SRS-22 scores) improved significantly compared to baseline.