INTRODUCTION
Cervical screw instrumentation has been widely utilized in the treatment of cervical spinal diseases for the promising great properties in the biomechanical stabilization, pullout strength, and protection of spinal cord and nerve roots [1,2]. However, the cervical region, an anatomically complex area, is adjacent to several vital structures, which are vulnerable to catastrophic complications from the malposition of cervical screws, including the neurological damage and vertebral artery injury [3]. Moreover, the anatomical morphology of cervical vertebrae is complicated by alterations due to the cervical fractures and congenital malformation, increasing the difficulty of cervical screw insertions [4,5]. Correspondingly, surgeons require years to gain sufficient experience to safely complete cervical screw instrumentation. Therefore, the demands for safety and accuracy of cervical screw placement drive advance in robot-assisted (RA) techniques on cervical spine surgery.
RA techniques have been widely and deeply investigated in thoracolumbar spine surgery, indicating promising clinical and radiographic outcomes [6-9]. However, studies on the application of RA methods in cervical spine surgery are still limited. In 2016, Tian [10] initially assessed the feasibility of TINAVI robot (TINAVI Medical Technologies, Beijing, China) for the posterior C1–2 transarticular screw placement in a case report, and concluded that the robotic guidance had a remarkable clinical potential in cervical spine surgery. Asuzu et al. [11] performed a percutaneous screw fixation of a hangman’s fracture under the guidance of the Mazor X robot (Mazor Robotics Ltd., Caesarea, Israel), and achieved accurate screw insertions with satisfactory fracture reductions. In another case report conducted by Farah et al. [12], 1 patient underwent C1–2 posterior percutaneous fixation using Cirq robot (Brainlab AG, Munich, Germany). Finally, all 4 screws were safely placed and rated as acceptable. In the 2020, Fan et al. [13] conducted the first randomized controlled trial (RCT) comparing TINAVI RA techniques with conventional freehand (FH) methods in terms of the accuracy of cervical screw placement. They found that the RA techniques showed superiority to FH methods in accuracy and clinical outcomes in cervical spine surgery. This finding is consistent with the conclusions obtained from the comparative studies performed by Su et al. [14], Lyu et al. [15], and Zhan et al. [16]. However, the rates of cervical screw placement accuracy with RA methods varied widely ranging from 66.7% to 91.4% in the published literatures of comparative studies and case series [13-19]. In addition, the application of RA system on cervical spine surgery is still in its early developmental stage, and whether the RA techniques are safe and accurate in cervical screw placement remains controversial.
Thus, this single-arm meta-analysis aims to demonstrate the safety and accuracy of cervical screw placement using the RA methods, which might provide references for surgeons in the selection of insertion methods and revolutionization of spinal surgeries, following improvement of RA techniques.
MATERIALS AND METHODS
1. Search Strategy
This research was performed in line with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [20]. The eligible studies were systematically searched from PubMed, Cochrane Library, Embase Database, Web of Science, Chinese National Knowledge Databases, and Wanfang Database without language restriction up to October 23, 2022. The following terms were searched in PubMed, Cochrane Library, Embase Database, and Web of Science: (“Cervical Vertebrae” [MeSH] or “Cervical Vertebra” or “Cervical Spines” or “Cervical Spine”) and (“Robotics” [MeSH] or robot or robotic). The keywords including “ji qi ren” and “jing zhui” were used in Chinese National Knowledge Databases, and Wanfang Database. The search strategy is shown in Supplementary Table 1. The inclusion of studies was determined by 2 reviewers, who independently screened the titles, abstracts, and full-text articles. Meanwhile, the reference lists and other relative studies were manually reviewed to identify additional worthy literature. Any disagreement was resolved by a third investigator.
2. Eligibility Criteria
The potentially relevant literatures were identified in accordance with the PICOS (Population, Intervention, Comparison, Outcomes, and Study) principle. The criterion of comparison was excluded due to the single-arm of this meta-analysis. (1) Population: The study population consisted of patients diagnosed with surgical indications in cervical spine. Studies involving cadavers or animals were excluded. (2) Intervention: RA techniques for cervical screw placement were performed in the single-arm or multi-arm studies. (3) Outcomes: Studies reporting the primary outcome, that is, the rate of cervical screw placement accuracy with robotic guidance, were eligible. Meanwhile, the subgroup analyses based on the screw type and insertion segments were performed. The assessment of screw position included the Gertzbin-Robbins [21], Rampersaud [22], and Ravi [23] criteria. The screw completely within the trajectory, without cortex breach, was regarded as an optimal position; the screw breaching the cortex by < 2 mm was considered clinically acceptable; the screw breaching the cortex by ≥ 2 mm indicated malposition. (4) Study design: RCTs, comparative cohort studies, and case series were included, whereas case reports, reviews, and conference reports were excluded in this study.
3. Data Extraction
The data were extracted by 2 pairs of independent reviewers from the qualified researches, and the controversies were settled by a third reviewer. The parameters, including the accuracy of screw insertion, the first author, the year of publication, study design, area, age, sex, body mass index (BMI), robot type, sample size, and number of screws were obtained to study the characteristics.
4. Qualitative Analyses
The methodological quality of included RCT was evaluated using the Cochrane risk of bias criteria [24]. In addition, the Newcastle-Ottawa Scale (NOS) criterion [25] was used to rate the risk of bias in the selected comparative cohort studies and case series. For the comparative cohort studies, quality assessment was performed in respect to patient selection, comparability, and outcomes with the total score of 9, and the scores more than 6 represent high quality. For the case series, the comparability questions from NOS criteria were removed, and the scores range from 0 to 7; the final scores more than 4 represent high quality. The qualitative analyses were independently conducted by 2 reviewers, and disagreements were resolved through discussion to reach consensus.
5. Statistical Analyses
The statistical analyses were performed using STATA 15.1 (StataCorp LLC, College Station, TX, USA). The pooled rate and its 95% confidence interval (CI) of summarized cervical screw placement accuracy was estimated by performing a meta-analysis of proportions using the cases with RA techniques in each study. Simultaneously, the pooled results of estimated blood loss during surgery and operation time were also calculated. The I2 at a significance level of p< 0.05 was utilized to evaluate the statistical heterogeneity, and the sensitivity and subgroup analyses were conducted to determine the source of heterogeneity. A p-value of < 0.05 was regarded statistically significant.
RESULTS
1. Literature Search
The process of literature selection for inclusion in this research is shown in Fig. 1. In the preliminary search from all databases, 740 studies were inspected. Moreover, 12 additional articles were identified through the reference lists and other relative studies. After duplicate elimination, 527 articles underwent title and abstract assessment, maintaining 16 studies for full-text screening. Finally, 1 RCT [13], 3 comparative cohort studies [14-16], and 3 case series [17-19] were included in our meta-analysis.
2. Characteristics of the Selected Studies
The baseline characteristics of the included studies are presented in Table 1. All 7 articles including 160 patients and 719 screws were newly published from 2020 to 2022. Among the included studies, 1 study was performed in Texas (the United States) [18], Marseille, (France) [17], Beijing (China) [13], Nanjing (China) [19], and Guangdong (China) [16]. The 2 remaining studies were conducted in Shanghai (China) [14,15]. The Mazor X Stealth/Medtronic [18] and Cirq/Brainlab [17] were used in one study, and the TiRobot/TINAVI [13-16,19] was reported in 5 studies.
3. Results of Qualitative Analyses
The quality of the RCT evaluated by Cochrane risk of bias criteria was moderate due to the high risk of blinding of participants and the personal and outcome assessment. Moreover, the 6 remaining studies were regarded as high quality, with 3 comparative cohort studies scored higher than 7, and 3 case series scored higher than 4, according to NOS criteria. The results of risk of bias for the selected studies are shown in Supplementary Tables 2, 3.
4. Outcomes of the Meta-Analysis
1) Accuracy of screw placement on cervical spine
A total of 719 cervical screws were placed in the 160 patients undergoing cervical spinal intervention with RA techniques. All the 7 studies [13-19] provided data on the optimal screw position that cervical screw was completely within the pedicle. The combined outcomes indicated that the rate of accuracy of cervical screw placement in RA methods was 88.0% (95% CI, 84.1%– 91.4%; p< 0.001; I2= 47.941%) (Fig. 2).
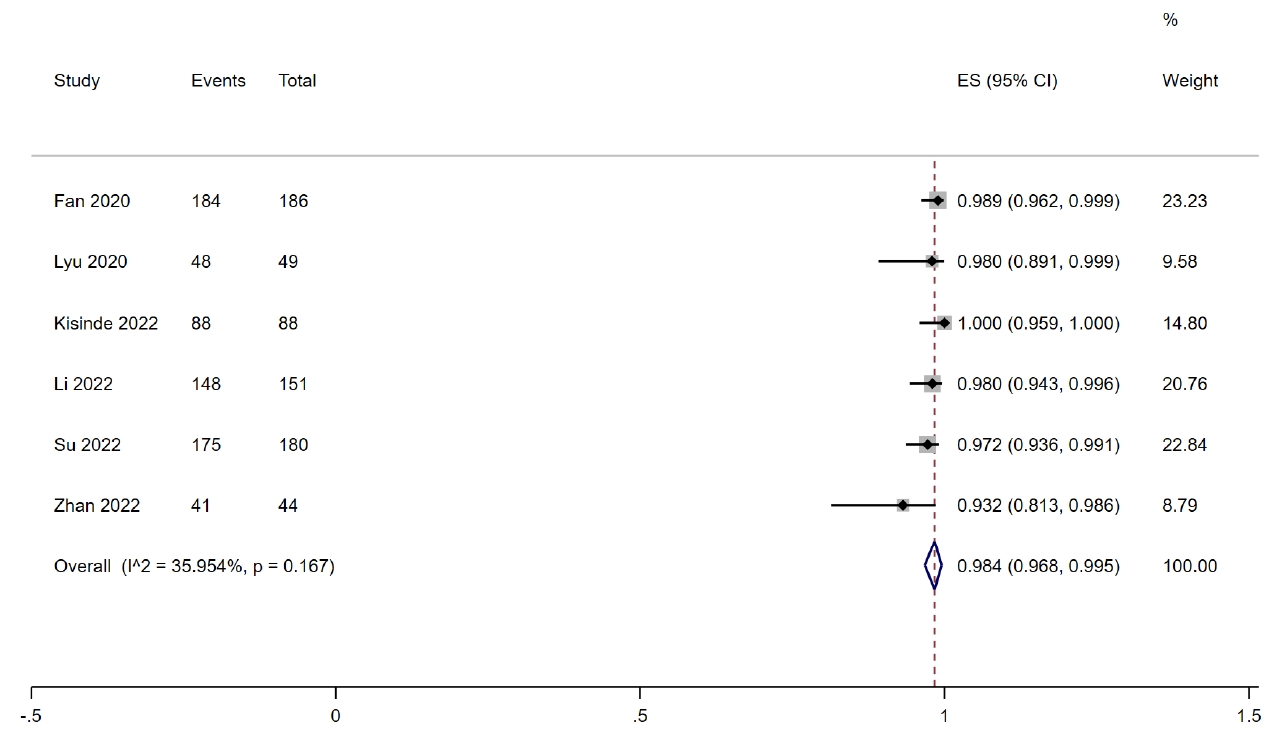
Seven studies [13-19] provided data on the clinically acceptable screw position that pedicle cortical breach was less than 2 mm. The combined results presented that the rate of clinically acceptable screw position with RA techniques was 97.8% (95% CI, 95.2%–99.5%; p< 0.001; I2= 63.713%) (Supplementary Fig. 1). Considering the significant heterogeneity (I2=63.713%, p=0.011), sensitivity analysis was performed. After the sequential removal of the included researches, the result indicated that the study of Farah et al. [17] led to the heterogeneity. After the exclusion of the study, the combined outcomes based on the remaining 6 studies [13-16,18,19] showed that the rate of clinically acceptable screw position was 98.4% (95% CI, 96.8%–99.5%; p< 0.001; I2= 35.954%) (Fig. 3).
2) Subgroup analyses of pedicle screw placement on cervical spine
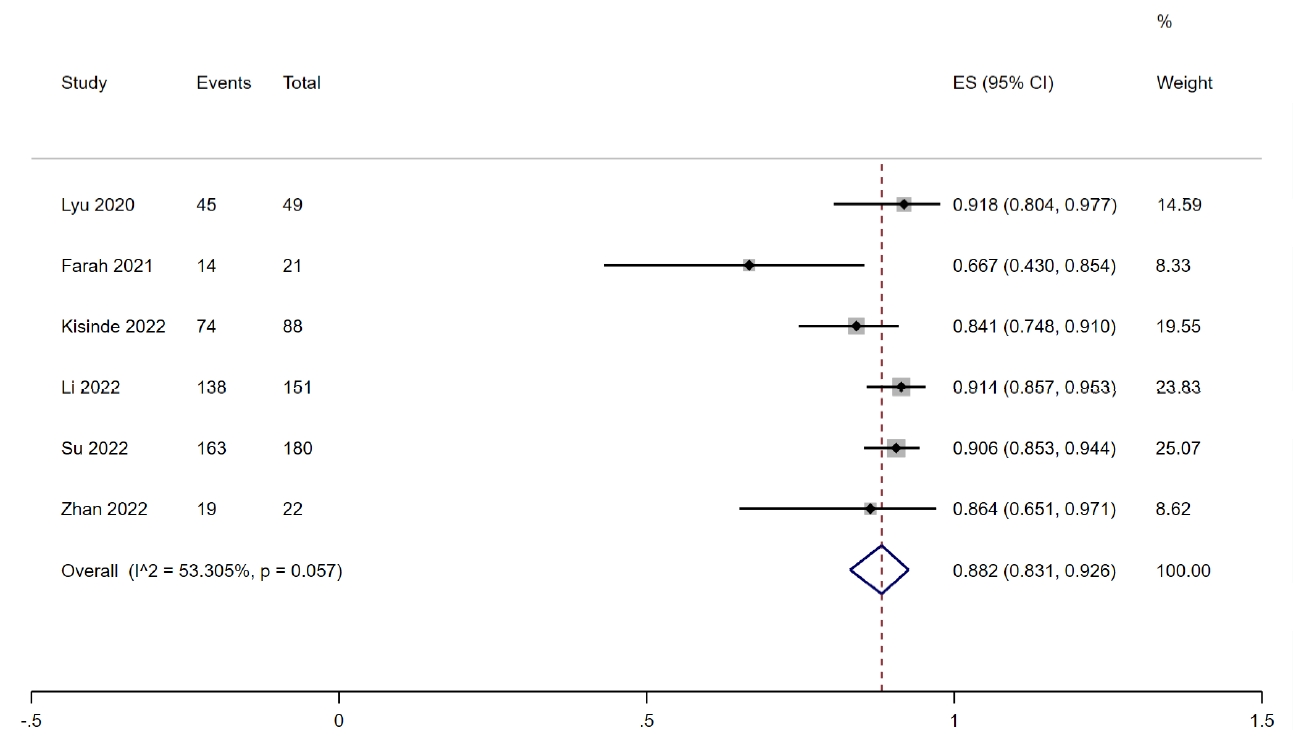
A total of 597 cervical pedicle screws were used in patients with RA techniques. The study of Fan et al. [13] with 86 pedicle screws was excluded due to the absence of illustration on the number of patients undergoing pedicle screws. Therefore, the combined outcomes based on the 6 studies [14-19] with 99 patients and 511 screws showed that with RA techniques, the rate of optimal pedicle screw position was 88.2% (95% CI, 83.1%–92.6%; p< 0.001; I2= 53.305%) (Fig. 4).
For the clinically acceptable pedicle screw position, the combined outcomes based on the 6 studies [14-19] showed that the rate of clinically acceptable screw position was 97.4% (95% CI, 93.6%–99.7%; p< 0.001; I2= 66.955%) (Supplementary Fig. 2). The heterogeneity was significantly high (I2= 66.955%, p= 0.010), which resulted from the study of Farah et al. [17] detected using sensitivity analysis. Finally, the combined outcomes based on the remaining 5 studies [14-16,18,19] with 92 patients and 490 screws indicated that the rate of clinically acceptable pedicle screw position was 98.4% (95% CI, 96.1%–99.8%; p< 0.001; I2= 42.156%) (Supplementary Fig. 3).
3) Subgroup analyses of accuracy of screw placement on C1 segment
Three studies [16,17,19] provided data on the screw position on C1 segment. The combined outcomes indicated that the rate of optimal screw position on C1 segment was 96.2% (95% CI, 80.5%– 100.0%; p< 0.001; I2= 44.134%) (Supplementary Fig. 4), and the rate of clinically acceptable screw position with RA techniques was 100.0% (95% CI, 98.0%–100.0%; p<0.001; I2=0.000%) (Supplementary Fig. 5).
4) Subgroup analyses of accuracy of screw placement on C2 segment
Three studies [16,18,19] provided data on the screw position on C2 segment. The combined results showed that the rate of optimal screw position on C2 segment was 89.7% (95% CI, 80.6%–96.6%; p<0.001; I2= 0.000%) (Supplementary Fig. 6), and the rate of clinically acceptable screw position with RA techniques was 97.1% (95% CI, 90.4%–100.0%; p< 0.001; I2= 0.000%) (Supplementary Fig. 7).
5) Subgroup analyses of accuracy of screw placement on subaxial cervical segments
Three studies [17-19] provided data on the screw position on subaxial cervical segments. The combined results showed that the rate of optimal screw position on subaxial cervical segments was 82.6% (95% CI, 70.9%–91.9%; p< 0.001; I2= 65.127%) (Supplementary Fig. 8), and the rate of clinically acceptable screw position with RA techniques was 96.4% (95% CI, 84.5%–100.0%; p< 0.001; I2= 83.735%) (Supplementary Fig. 9).
DISCUSSION
The application of RA techniques in the cervical spine surgery remains relatively nascent compared with that in thoracolumbar regions, because the surgery on cervical spine, especially the upper cervical spine, is almost the most complex and risky spinal surgery with steep learning curve [10]. Recently, RA techniques have been increasingly utilized in cervical spine surgery, showing promising accuracy of screw insertion. In the RCT performed by Fan et al. [13], 87.6% of the 186 cervical screws in RA groups were graded as optimal position, whereas this proportion in FH group was only 60.8% in 204 cervical screws. Su et al. [14] prospectively enrolled 58 patients and 374 cervical pedicle screws in RA and FH cohorts, respectively, and demonstrated that the rate of optimal accuracy of screw insertion was remarkably higher in the RA group (90.6%) than that in the FH group (71.1%). In the 2 retrospective cohort studies, the accuracies of cervical screw placement were 84.1%–91.8% and 49.2%–73.2% in RA and FH groups, respectively [15,16]. Our meta-analysis demonstrated that the rates of optimal and clinically acceptable screw positions in RA techniques were 88.0% and 98.4%, respectively. Moreover, cervical pedicle screw placement has been widely used due to the biomechanically satisfactory fixation and pullout strength. Thus, the subgroup analysis based on the cervical pedicle screws were also performed. We found that for pedicle screws, the rates of optimal and clinically acceptable screw positions with RA methods were 88.2% and 97.4%, respectively, showing promising insertion accuracy. The combined outcomes indicate that the RA techniques are feasible and safe in cervical screw placement, as explained in the follow statements. First, robotic system can identify the ideal entry point and trajectory for accurate screw insertion based on the 3-dimensional (3D) computed tomography (CT) reconstructions [26]. In the trajectory view, the RA techniques were reported to deviate screws from preoperative planning by 1.32± 1.17 mm in the axial plane and by 1.27± 1.00 mm in the sagittal plane with low rate of cortical breaches [18]. However, for the conventional FH methods, the entry point and trajectory are assessed through x-ray fluoroscopy, and the accuracy of screw insertion depends heavily on the surgical experience and skills of surgeons. Moreover, cervical fractures and congenital malformation in patients increase the operative difficulty in FH methods. Thus, the RA technique can reduce human error and the rate of malposition. In addition, the robotic system is associated with high stability on the accurate insertion. Surgeons might experience fatigue due to the long surgical time and complex operation in traditional FH procedures, thereby increasing the likelihood of malposition. By contrast, RA methods have reliable reproducibility and fatigue resistance, further improving the safety and accuracy in cervical spine surgery.
Computer-assisted navigation (CAN) techniques have also been applied as an alternative selection to improve the insertion accuracy. Chachan et al. [27] prospectively included 241 cervical screws under the O-arm based CAN, and found that 92.95% of the screws caused no pedicle breach. Moreover, none of the screws resulted in neurovascular injury, showing promising clinical outcomes. Meanwhile, Gan et al. [28] and Zhang et al. [29] drew similar outcomes that 22.9% and 29.7% of the cervical screws with CAN breached the pedicles but without intraoperative or postoperative complication caused by malposition. However, in the study of Farber et al. [30], CAN cohort did not present remarkably improved rate (64.0%) of accuracy in transpedicular screw placement compared with the direct visualization group (88.0%) in the subaxial cervical pedicle screw insertion. Our meta-analysis showed that the accurate rate of cervical screw placement with RA techniques was 88.0%, which was higher than the results of insertion accuracy with CAN reached by Gan et al. [28] (77.1%), Zhang et al. [29] (70.3%), and Farber et al. [30] (64.0%). With CAN techniques, the position of screw during insertion procedures can be tracked real time. However, the entry point and trajectory are ultimately determined by surgeons, requiring rich surgical experience and professional judgment based on the 3D imaging [27]. In addition, the attention of surgeon is easily distracted from screw insertion when focusing on the navigation screen. Thus, remarkable hand-eye coordination is required with CAN methods [31]. Meanwhile, the surgeons should maintain stable arm as much as possible during the operation because the cervical segments are not rigidly connected to the navigation recognition frame; thus, they are prone to errors due to relative motion [19]. By contrast, the entry point and trajectory were automatically identified in RA methods, which required short learning curves for surgeons [32]. Moreover, the arm of the robotic system can operate in a real-time dynamic compensation mode, thereby reducing error-prone movements and improving insertion accuracy.
The anatomical morphologies of atlas, axis, and subaxial cervical vertebrae varied largely, probably resulting in outcome bias on the accurate rate of cervical screw placement. Therefore, the subgroup analyses on cervical segments of C1, C2, and subaxial cervical vertebrae were conducted to determine the influence of cervical levels on the accuracy of screw insertion. The current study has demonstrated that the rates of optimal screw positions on C1, C2, and subaxial cervical segments with RA techniques were 96.2%, 89.7%, and 82.6%, respectively, which were broadly consistent with previous studies. In the study of Li et al. [19], the rates of optimal pedicle position on C1 and C2 with RA techniques were 97.06% and 91.67%, respectively, whereas the rate of subaxial levels was 88.3%, and the lowest rate of accuracy was 71.4% on C4. Mao et al. [33] performed RA cervical screw placements on C2–C7 segments in 4 cadaver specimens. They found that the rate of breach on C2 was 16.6%, whereas the breach distributions on C3–C7 were 71.4%, 66.6%, 50.0%, 33.3%, and 25.0%. Moreover, they further analyzed the anatomical metrics, demonstrating that the mean pedicle height was largest in C2, and the pedicle width of C2 was larger than those of C3 and C4. Thus, the accuracy of screw placement on C2 was higher than that on subaxial segments. Furthermore, the mean width of C1 lateral mass was 13.7 mm, as reported by Lin et al. [34]; it was larger than that of C2 lateral mass (9.9 mm), which was measured by Ji et al. [35], presenting larger safe zones for screw insertion in the atlas. Moreover, the limitation of pedicle screw utilization on C2 was the pedicle width with the average lengths of 5.50 and 3.97 mm at the middle and lower parts; whereas the limitation of pedicle screw utilization on C1 was the posterior vertebral groove height with the average length of 4.9 mm [34,36]. Furthermore, a study by Huang et al. [37] further revealed that a 3.5- or 4.0-mm-diameter screw can be safely inserted into the C1 pedicle with the posterior vertebral groove height less than 4.0 mm, when the C1 pedicle has a medullary canal. Therefore, the rate of cervical screw placement on C1 level might be higher than that on C2 segment.
Robotic systems in cervical spine surgery also showed promising clinical outcomes compared with FH methods, including less blood loss during surgery and shorter length of hospital stay after surgery [13,16]. Menger et al. [38] reported that the application of RA methods on spine surgery was cost-effective with less revision surgery and low infection rate. In the current study, we have found that the combined blood loss during surgery was 197.67 mL, and the combined operation time was 268.88 minutes with RA methods. In addition, RA methods were associated with remarkably less radiation time and radiation dose to patients and surgeons than conventional FH methods [14-16]. In the conventional FH cervical surgery to guarantee insertion accuracy, the fluoroscopies were repeatedly performed to adjust the screw deviation. RA methods mainly required preoperative planning with 3D CT scans and postoperative verification with a fluoroscopy in a fast speed. Lieberman et al. [39] reported that the RA methods might reduce 40% to 70% intraoperative radiation exposure for patients, surgeons, and operating-room personnel compared with the FH methods. Regarding the clinical outcomes under robotic guidance, further studies are required to assess the utility in the future work.
There are potential risks of RA cervical instrumentation. The drift and deviation are very important risk in all cervical posterior instrumentation surgery. The drift and deviation of cervical screws from preplanned entry point and trajectory due to pressure of soft tissues and irregular bony surfaces might cause insertion errors, which increase the risk of neurological and vascular complications [31]. Meanwhile, the cervical spine easily bends, and 3 levels away from the reference tracker were the risk factors for malposition in not only RA pedicle screw placement but also CAN method. Moreover, the imaging software in the robotic systems should be updated and enhanced for better image registration and reduction of the draft from tidal volume during mechanical ventilation [40]. The slight deviation causing no complications in thoracolumbar insertion might contribute to fatal consequences in cervical instrumentation, the avoidance of which demands elevated technical innovation. Besides, according to a study by Zhang et al. [41], among 163 patients and 780 screws, severe obesity (BMI≥ 30 kg/m2), osteoporosis, and segments 3 levels away from the tracker were the risk factors for malposition in RA pedicle screw placement. Furthermore, the penetration level of robotic systems is still relatively low due to the expensive robotic equipment for hospitals and high medical expenses for patients. In addition, serious complications such as neurovascular injury and cerebrospinal fluid leakage due to the screw fixations might result in catastrophic consequences. In the current research, 6 of the included 7 studies reported the complications due to RA screw malposition, but no serious complications were observed in the 6 literatures [14-19]. Thus, the meta-analysis on the complications was not performed.
The challenges, including the technical difficulties, fiscal investment, learning curves, and minor improvements in clinical outcomes, would inevitably arise in the penetration and popularity of a new technology [42]. With modification and revolution of skills and techniques, the RA techniques not only expand the approaches to cervical surgery, but also redefine the concept of cervical surgery [43]. For instance, RA methods conform to the minimal invasion and rapid rehabilitation surgery concept. Patients suffering from the displaced atlas fractures could receive the minimally invasive percutaneous lag screw insertion with RA methods for rapid rehabilitation, instead of the traditional medical interventions of external reduction with skull traction and immobilization with a Halo-vest. Furthermore, the real-time remote surgery can be implemented based on fifth generation wireless system (5G) and RA techniques. Tian et al. [44] assessed the efficacy and feasibility of 5G telerobotic spinal surgery on 12 patients with spinal disorders, concluding that 5G remote RA surgery is accurate and reliable with safety. In the assistance with 5G remote RA application, patients requiring cervical surgery in emergency can nearby receive remote intervention from surgeons with excellent skills and rich experience, and patients in remote rural areas can receive spinal surgery conducted by experts worldwide. At present, the robotic systems only work as assistive tools for accurate insertion, but the spinal robots might transform as a major or an independent surgical operator with the development of robotic technology in the future.
Several potential weaknesses of this meta-analysis exist. First, the current single-arm meta-analysis has only demonstrated the safety and accuracy of RA cervical screw placement without the conventional FH methods as control group. Only a few studies compared RA and FH methods in terms of the clinical and radiographic outcomes because the robotic guidance on cervical spine is still a new clinical and applied technique. Thus, the meta-analysis comparing the 2 methods cannot be performed. Nevertheless, this research presented the safety and feasibility of RA cervical screw and provided references for surgeons and technologists. Second, 5 studies were conducted in China. However, the 5 studies were performed in 4 different areas with large geographical distances, which might not bias the combined outcomes of this study in terms of the publication areas. Third, the clinical outcomes, including the blood loss during surgery and operation time, might be biased due to surgical segments, the number of inserted screws, and the number of surgical levels. Thus, the meta-analyses on these clinical results were not performed. Fourth, only 7 studies with 160 patients and 719 cervical screws were included. More RCTs and prospective cohort studies with large samples were urgently required for high levels of evidence to support this recommendation.