Independent Correlation of the C1–2 Cobb Angle With Patient-Reported Outcomes After Correcting Chronic Atlantoaxial Instability
Article information

Abstract
Objective
To investigate three-planar radiographic results and patient-reported outcomes (PROs) after correcting chronic atlantoaxial instability (AAI) by translaminar screw (TLS) and pedicle screw (PS) fixation, and to explore the potential association of atlantoaxial realignment with PRO improvements.
Methods
Twenty-three patients who underwent C1 lateral mass screw (LMS)-C2 TLS and 29 who underwent C1 LMS-C2 PS with ≥ 2 years of follow-up were retrospectively analyzed. Three-planar (sagittal, coronal, and axial) radiographic parameters were measured. PROs including the Neck Disability Index (NDI), Japanese Orthopaedic Association (JOA) score and the Short Form 36 Physical Component Summary (SF-36 PCS) were documented. Factors potentially associated with PROs were identified.
Results
The radiographic parameters significantly changed postoperatively except the C1–2 midlines’ intersection angle in the TLS group (p = 0.073) and posterior atlanto-dens interval in both groups (p = 0.283, p = 0.271, respectively). The difference in bilateral odontoid lateral mass interspaces at last follow-up was better corrected in the TLS group than in the PS group (p = 0.010). Postoperative PROs had significantly improved in both groups (all p < 0.05). Thereinto, NDI at last follow-up was significantly lower in the TLS group compared with PS group (p = 0.013). In addition, blood loss and operative time were obviously lesser in TLS group compared with PS group (p = 0.010, p = 0.004, respectively). Multivariable regression analysis revealed that a change in C1–2 Cobb angle was independently correlated to PROs improvement (NDI: β = -0.435, p = 0.003; JOA score: β = 0.111, p = 0.033; SF-36 PCS: β = 1.013, p = 0.024, respectively), also age ≤ 40 years was independently associated with NDI (β = 5.40, p = 0.002).
Conclusion
Three-planar AAI should be reconstructed by C1 LMS-C2 PS fixation, while sagittal or coronal AAI could be corrected by C1 LMS-C2 TLS fixation. PROs may improve after atlantoaxial reconstruction in patients with chronic AAI. The C1–2 Cobb angle is an independent predictor of PROs after correcting chronic AAI, as is age ≤ 40 years for postoperative NDI.
INTRODUCTION
Atlantoaxial instability (AAI) is a complicated clinical syndrome with excessive movement at atlantoaxial junction, which may result from trauma, degeneration, congenital anomaly, infectious or neoplastic lesions, etc [1-4]. AAI could result in patients’ neurological deficits by compression on spinal cord or nerve root [5,6]. Decompression, reduction and fusion are recommended to treat AAI because the persistent upper cervical instability may cause a risk of progressive myelopathy [7].
Researchers revealed that wiring technique decreased atlantoaxial fusion rate as lacking rigid immobilization [8], while transarticular screw fixation increased the risk of vertebral artery injury [9]. Wright and Lauryssen [10] reported a 20% incidence of cervical vertebral anomalies and led to the misplacements of transarticular screw in clinic. Compared with pars screw, pedicle screw (PS) and translaminar screw (TLS) both provide a stronger anti-pullout strength between the interface of bone and screw [11]. Imperfectly, on the one hand PS fixation possesses the strongest fixation in spine surgery, on the other hand PS insertion brings about a relative high incidence of injuries to nerve root and vertebral artery in the atlantoaxial joint [12,13]. Correspondingly, Dorward and Wright [14] demonstrated that TLS fixation could act as an alternative technique to treat AAI, and salvage the AAI patient with dysplastic pedicle or ectopic vertebral artery. Further compared with PS fixation, C2 TLS fixation has no significant differences in fusion rate, revision rate and total complications after atlantoaxial reconstruction [15-17].
To date, most of the studies referring to fixation with screw and rod just focused on reporting biomechanical and uniplanar radiological outcomes. To our knowledge, it is currently short of reporting 3-planar (sagittal, coronal, and axial) radiological outcomes after atlantoaxial reconstruction, but any planar instability may lead to neurological deficits, also no literature has revealed the chronic AAI patients’ postoperative patient-reported outcomes (PROs) which on behalf of quality of life. Furthermore, is there a potential association between cervical reconstruction and improvements of PROs? Hence, this study aimed to (1) investigate the three-planar radiographic results and PROs after correcting chronic AAI by TLS fixation and PS fixation, (2) explore the potential association between atlantoaxial reconstruction and improvements of PROs.
MATERIALS AND METHODS
Seventeen females and 35 males who had AAI at sagittal, coronal, or axial plane were enrolled in this retrospective 3-center study between July 2011 and January 2016. Of these, 23 patients with bilateral C1 LMS-C2 TLS fixation and 29 patients with bilateral C1 LMS-C2 PS fixation were compared. Inclusion criteria for chronic AAI were adult patient with neurological symptom greater than 3 months and atlanto-dens interval (ADI) greater than 3 mm on radiograph, or he/she had excessive movement at C1–2 joint on flexion and extension radiographs of the neck, which as a result of either a bony or ligamentous abnormality derives from trauma, degenerative change, congenital cause, inflammation or tumor, etc. And patient’s neurologic symptoms such as occipitocervical pain and/or numbness as well as stiff neck can occur when spinal cord or nerve roots were involved and revealed on imaging findings. Besides, inclusion criteria in TLS group still include AAI patients with ectopic vertebral artery (Fig. 1A, B), or dysplastic C2 pedicle with inner diameter ≤3.5 mm, mid laminar thickness ≥4.0 mm and craniocaudal laminar length ≥8.0 mm, or excessive convergent C2 pedicle. If patient’s anatomical parameters beyond these criteria, or severe osteoporosis as well as severe kyphotic case were excluded. Inclusion criteria in PS group still include AAI patient with C2 inner pedicle diameter >3.5 mm [18], and with normal vertebral artery, but the cases with ectopic vertebral artery or dysplastic pedicle were excluded. Patients’ demographics and etiologies were summarized in Table 1.
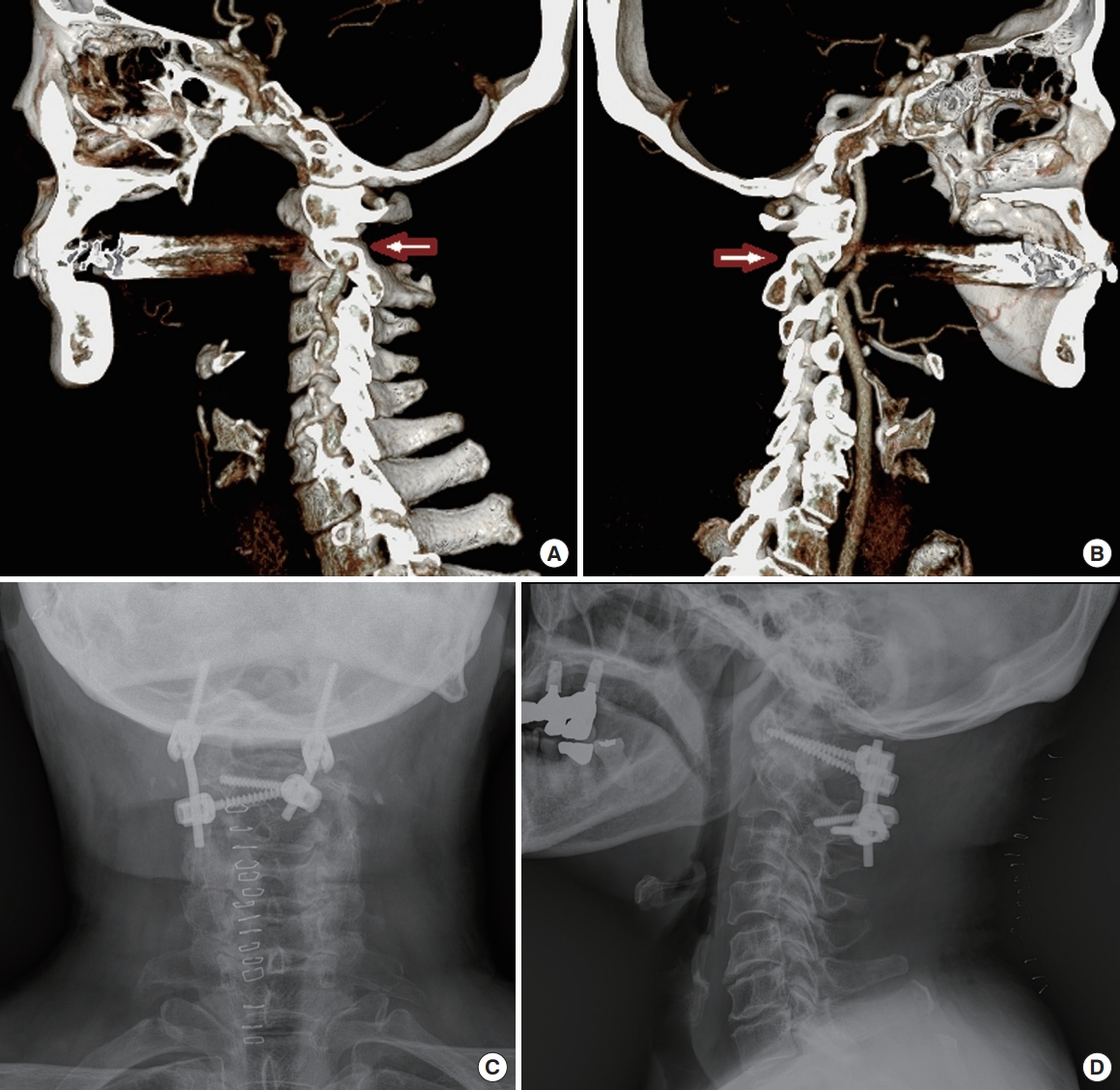
A patient with chronic atlantoaxial instability (AAI) underwent C2 translaminar screw fixation. (A, B) Computed tomography reconstruction images showed atlantoaxial sagittal malalignment and bilateral high-riding vertebral arteries (arrow). (C) Postoperative posteroanterior radiography showed the crossing C2 translaminar screws fixation. (D) Sagittal radiography showed atlantoaxial realignment after surgery.
Demographics and etiologies
The chronic AAI was diagnosed by computed tomography (CT) scan, patient’s disease course, neurologic symptoms and signs. Preoperative CT scan detected cervical anatomical structures, CT angiography was used to confirm the course of the vertebral artery. To reduce clinical heterogeneity and confounding factor, consistent surgical procedures were conducted by three seasoned surgeons from three spine centers. This study was reviewed and approved by the Institutional Review Board of Yonsei University College of Medicine (approval number: 4-2017-0209), informed consents were obtained from eligible patients.
1. Operation, Postoperative Care and Follow-up
C1 LMS was placed according to Harms’s technique [19], C2 TLS was inserted by Wright’s technique [20]. (Fig. 1C, D) Antimicrobials and painkiller were routinely administrated in patients for 24 hours and 72 hours postoperatively. Patient wore a hard cervical collar for 12 weeks after surgery. Operative time, blood loss, fusion rate, neurological deficits and relevant complications were recorded to further evaluate surgical safety and efficiency. Bone graft was placed in the interlaminar space to facilitate bony fusion. With CT scans, we routinely checked dynamic fusion by different point-in-time such as one month, three months, six months, twelve months, and twenty-four months postoperatively. The criteria used to determine fusion on plain x-ray or CT scans were that (1) the bone in fusion area was more dense than originally achieved during surgery, (2) no space between graft bone and autologous bone, and (3) mature bony trabeculae bridging in fusion area. In addition, all patients achieved follow-up in an average of 31 months (range, 24–39 months).
2. Radiographic Measurements
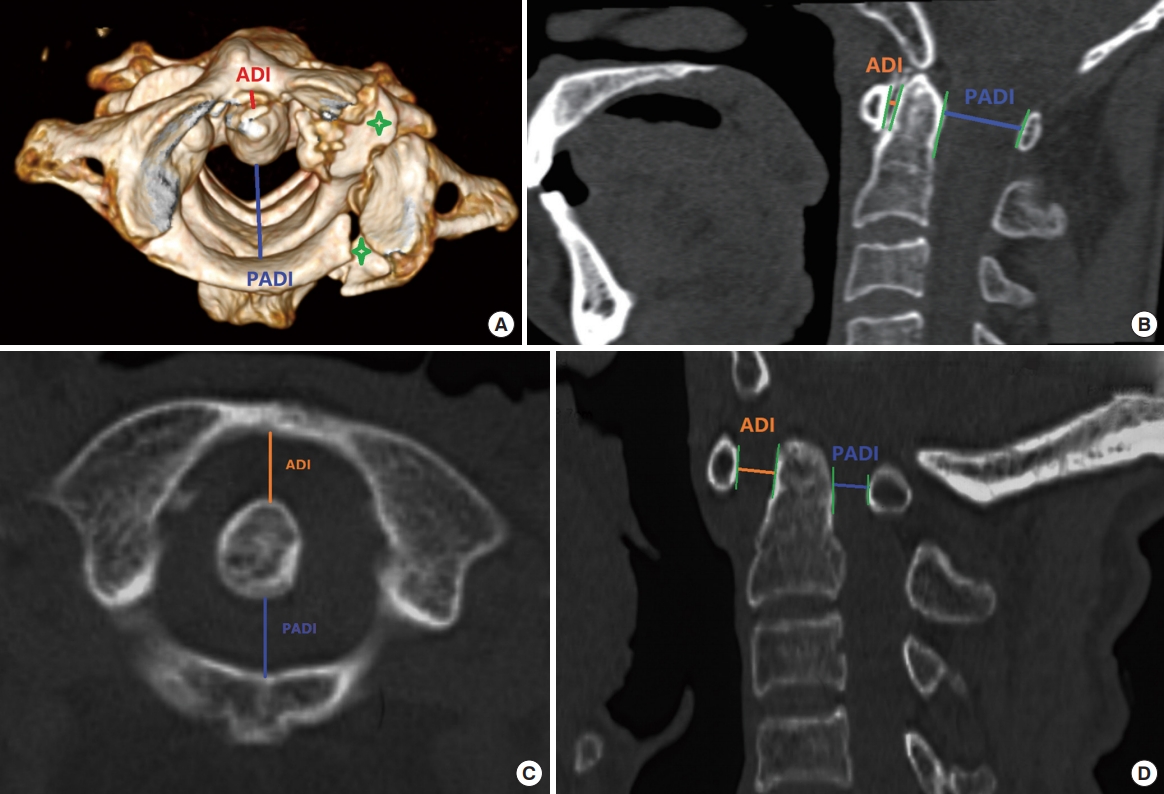
Preoperative cervical radiography and CT scans were routinely taken for patients’ surgical plans. Postoperative CT scan was used to reveal bony fusion, hardware position. Postoperative radiographic parameters were routinely recorded at 2 years’ follow-up for data analyses. The ADI, posterior ADI (PADI), basion-dental interval (BDI), basion-posterior axial line interval (BAI), C1–2 Cobb angle and center of gravity of head to C7 sagittal vertical axis (CGH-C7 SVA) were measured to describe cervical sagittal alignment (Fig. 2A, B). Of these, ADI is the distance from a line drawn along midpoints of anterior ring of C1 to another line drawn down along anterior edge of odontoid process. PADI is the anteroposterior diameter of the spinal canal at ADI level. BDI is the interval from the most inferoposterior point of the basion to the superior tip of odontoid process. BAI is the interval from the most inferoposterior point of the basion to the extensional line drawn along posterior edge of odontoid process. The C1–2 Cobb angle was defined as the angle between a line connecting superior margin of C1 anterior tubercle to superior margin of C1 spinous process and the other line along C2 inferior endplate. CGH-C7 SVA was defined as the distance between CG plumb line (extending from anterior margin of the external auditory canal) and posterosuperior point on endplate of C7.
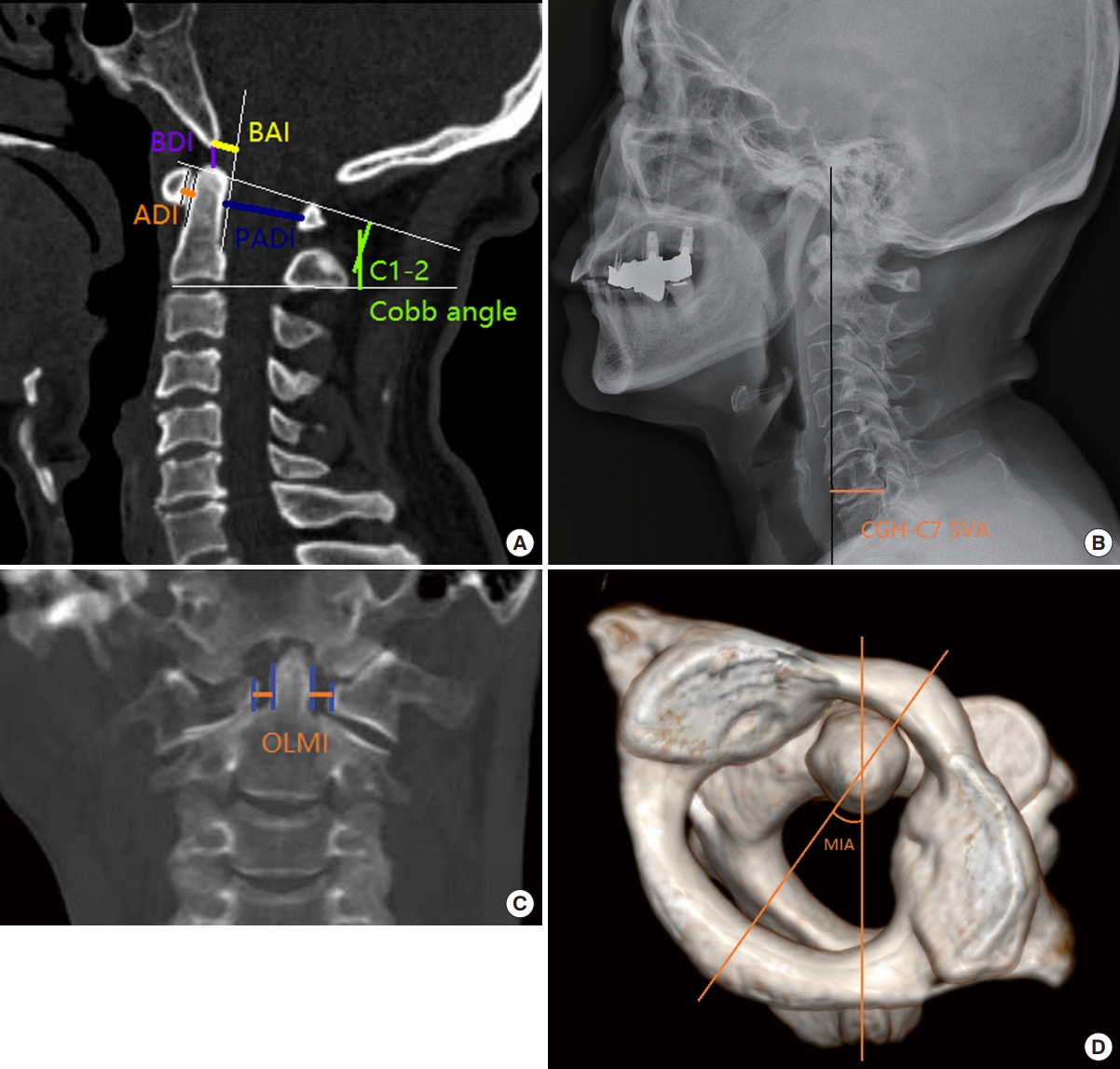
Three-planar radiographic measurements. (A) atlanto-dens interval (ADI), posterior ADI (PADI), basion-dental interval (BDI), basion-posterior axial line interval (BAI), and C1-2 Cobb angle are measured on sagittal plane. (B) center of gravity of head to C7 sagittal vertical axis (CGH-C7 SVA) is measured on sagittal plane. (C) odontoid lateral mass interspaces (OLMI) is measured on coronal plane. (D) C1-2 midlines’ intersection angle (MIA) is measured on transverse plane.
In addition, difference between bilateral odontoid and lateral mass interspaces (ΔOLMI) was measured to describe atlantoaxial coronal reconstruction. The interspace is between the lateral aspect of odontoid and the medial aspect of massa lateralis atlantis (Fig. 2C). C1 and C2 midlines’ intersection angle (MIA) represents a rotatory angle on C1–2 plane (Fig. 2D): a line pass through the center of C1 anterior tubercle and posterior tubercle (line 1), the other line pass through the midpoint of C2 spinous process and odontoid (line 2), the intersection angle between lines 1 and 2 was named MIA.
3. Evaluation of PROs
Pre- and postoperative neurological statuses in all patients were recorded by PROs to reveal patients' quality of life. Thereinto, Neck Disability Index (NDI) is a neck pain-specific PROs for indicating how neck pain affects a patient’s ability in daily life [21]. Japanese Orthopaedic Association (JOA) score is a generalized assessment on cervical spinal cord’s functional status including ambulation, sensation and muscular tension [22]. While 36-Item Short Form (SF-36) is an integrated questionnaire that counts self-perceived general health by 8 health status subscales [23].
4. Statistical Analysis
All statistical analyses were performed by IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA). Data were presented as mean±standard deviation. A probability less than 0.05 was considered statistically significant. Preoperative and follow-up data were compared by paired t-test. Independent-samples t-test was used to compare corresponding data between the 2 groups. Multiple regression analysis with Enter method was carried out to assess the individual variable contribution to PROs.
RESULTS
All the enrolled 52 patients (23 patients performed TLS fixation vs. 29 patients performed PS fixation) finally achieved bony fusion and their incisions healed primarily, no instrumentation was loosened or rupturing after surgery. Of these, one patient in TLS group suffered delayed union (the fracture was healed in 7 months postoperatively). One patient from PS group occurred postoperative occipitocervical pain and limited movement due to the injury on C2 nerve root. The patient’s neurological deficits got well after a revision surgery by replacing a TLS (NDI decreased from 45 to 7, JOA score improved from 10 to 15). Another case in PS group occurred a vertebral artery injury due to a C2 PS penetrated a transverse foramen, the bleeding had been prevented intraoperatively. The neurovascular injury rates were 0 in TLS group vs. 6.9% in PS group (p=0.577). Additionally, an average of 173±80 mL blood loss was in TLS group and 256±108 mL in PS group, respectively (mean difference [MD], 83 mL; 95% confidence interval [CI]: 139–208 mL vs. 209–302 mL, p=0.010). A mean of 90±23 minutes operative time was in TLS group vs. 117±29 minutes in PS group (MD, 27 minutes; 95% CI: 80–100 minutes vs. 104–129 minutes; p=0.004).
1. Radiographic Outcomes
Radiographic parameters for patients in TLS and PS group were summarized in Table 2. Of the parameters, except PADI in both group and MIA in TLS group had no significant changes after surgeries, the remaining radiographic parameters were significantly corrected after surgeries in both group (all p<0.05). Without significant difference existed in both groups’ preoperative radiographic parameters (all p>0.05). And except ΔOLMI, there was no significant difference in other radiographic results between both groups’ last follow-up. Compared with PS fixation, TLS fixation was superior in coronal correction for realigning AAI (ΔOLMI, 1.0±0.6 mm vs. 1.5±0.7 mm, p=0.010), but it was inferior to PS fixation on transverse correction from preoperatively to postoperatively (C1–2 MIA, p=0.073 vs. p=0.004).
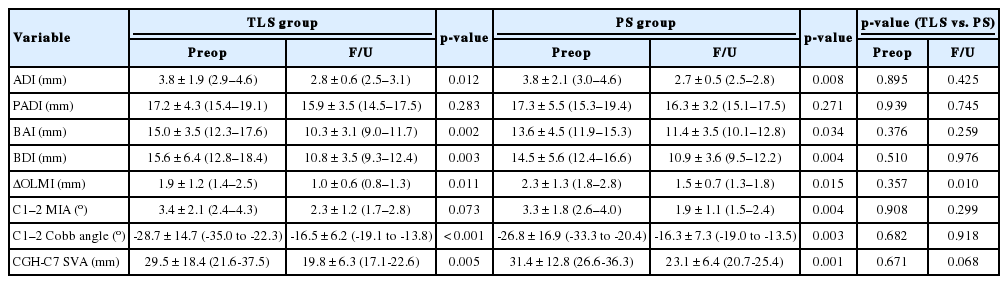
Preoperative and 2-year follow-up radiographic results in TLS and PS groups
2. PROs and the Associated Factors
As shown in Table 3, NDI, JOA score and Short Form 36 Physical Component Summary (SF-36 PCS) significantly improved from preoperatively to last follow-up in both groups (all p<0.05, postoperative 24 months). Compared with PS group, the NDI was improved better in TLS group at last follow-up (11.4±4.8 vs. 16.0±7.7, p=0.013).

Preoperative and follow-up patient-reported outcomes in TLS and PS groups
The potential factors correlated with improvements of PROs were explored by multivariable regression analysis with Enter method (Table 4). We found that postoperative C1–2 Cobb angle was the independent influential factor related to postoperative NDI, JOA score, and SF-36 PCS (p=0.003, p=0.033, and p=0.024, respectively). On basis of our clinical experiences, a range of -16.0°±7.0° might be the optimal postoperative C1–2 Cobb angle for improving patients’ quality of life (Table 2). Additionally, patients ≤40 years of age independently correlated with postoperative NDI (p=0.002).
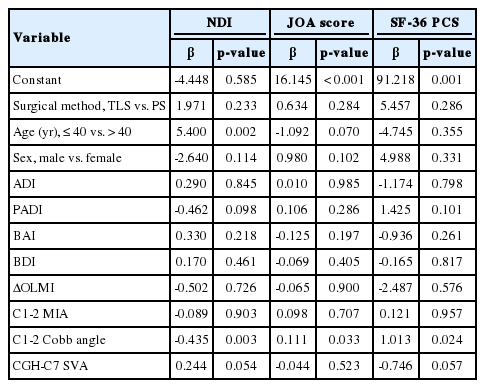
Potential associative factor correlated with postoperative patient-reported outcomes (multivariable regression analysis)
DISCUSSION
Majority of upper cervical instabilities occur at atlantoaxial complex and may lead to neurological deficits [24], in particular to the 3-planar fractures associated with high rates in neural morbidity and mortality [25]. Among the available atlantoaxial instrumentations, PS fixation provides strong antipullout strength between the interface of bone and screw [11], while TLS technique can balance rigid fixation and surgical safety [11,15,16]. However, there is no literature has reported 3-planar radiographic results and PROs after correcting AAI. In this study, we compared the properties of C1 LMS-C2 TLS fixation and C1 LMS-C2 PS fixation by treating chronic AAI, and found that there was no significant difference in neurovascular injury, bony fusion, PROs, and majority of radiographic results. However, TLS fixation was inferior to PS fixation on atlantoaxial transverse correction but it was superior in coronal reconstruction. In addition, we found that C1–2 Cobb angle is an independent factor relates to improvement of PROs after correcting chronic AAI.
1. Radiographic Findings
In this study, radiographic parameters were measured on basis of cervical spinal sagittal, coronal and axial planes. On sagittal plane, ADI is an indication for ligamentous integrity [26]. ADI >5 mm in adults indicates the misalignment of C1 lateral masses necessitates reduction [27]. With marked reproducibility, PADI >13 mm is an indication for nonoperative treatment if displaced odontoid fracture occurs in elderly patients [28]. While BDI and BAI are acting as the supplemental measurements for ADI and PADI in cases of type II or III of Anderson and D’ Alonzo odontoid fractures. Harris et al. [29] measured BAI and BDI on sagittal radiographs from 400 normal adults and found both ≤12 mm were in 98% and 95% of adults. On coronal plane, ΔOLMI is an indication for atlantoaxial subluxation and should be routinely evaluated for spreading of C1 lateral mass [30,31]. Sutherland’s investigation revealed a mean difference value of 1.2±0.8 mm was the asymmetry of OLMI in nonrotated specimens [32]. Lastly, given that half cervical rotations come from atlantoaxial articulation, we used C1–2 MIA to compare pre- and postoperative rotational alignment.
Most radiographic parameters were significantly improved after surgeries in the participants except C1–2 MIA in TLS group and PADI in both group (Table 2). As for postoperative “unchanged” PADI, we traced the reason and found that preoperative anteroposterior diameters of atlantoaxial spinal canals were disordering in many AAI cases due to broken and outspread C1 rings (enlarged PADI) or enlarged ADI in normal or compressed C1 rings (shortened PADI) (Fig. 3), the mixture of enlarged and shortened PADI resulted in an average preoperative PADI was close to normal value. Hence, there was no significant change in the average value of PADI after surgery. With respect to the unsignificant change of C1–2 MIA in postsurgical TLS group, the reason might be that TLS fixation was inferior to PS fixation in restoring rotatory C1–2 displacement (Table 2). But it seemed that TLS fixation was superior to PS fixation in correcting coronal malalignment (follow-up ΔOLMI, 1.0±0.6 mm vs. 1.5±0.7 mm, p=0.010).
Variation of posterior atlanto-dens interval (PADI). (A, B) PADI was enlarged due to C1 separation fracture (asterisk). (C, D) PADI was decrescent due to enlarged atlanto-dens interval (ADI) in the atlas (C1) with normal anteroposterior diameter.
2. PROs and Correlated Factors
PROs were significantly improved after surgeries in both groups (Table 3). Because the longstanding malalignment derived from chronic AAI could lead to cervical extensors’ fatigue/pain (high NDI) [33], actually, any planar dislocation resulted in compression on neurologic element might generate poor PROs preoperatively. While relief of these sufferings came up after surgeries, which improved patients’ PROs at different levels. However, compared with postoperative NDI and JOA score, postoperative SF-36 PCS improved not so obviously, this might result from its property of non–neck-specific assessment.
Multivariable regression analysis (Enter method) revealed that C1–2 Cobb angle was the independent factor related to PROs after atlantoaxial reconstruction (Table 4), and patients ≤40 years of age independently correlated with NDI. Correspondingly, Yudoyono et al. [34] found that C1–2 Cobb angle was significantly changed after C1–2 fixation in patients with os odontoideum, also visual analogue scale and JOA score were improved postoperatively. These results enlighten us that atlantoaxial sagittal reconstruction may be critical to improve PROs.
3. Limitations
There were several limitations in this study. First, although we measured 3-planar radiographic parameters, so far, there is no standardized measurement for all-sided assessments on atlantoaxial alignment. Of the radiographic parameters, MIA was used in our clinical evaluation for measuring cervical rotation, but lacking of accurate reference value to assess normal/abnormal rotational angulation. Second, the positions of imaging exams for individual patient had not been consistently performed from pre- to postoperatively, which was an unmanageable factor in retrospective study but might result in radiographic parameters’ biases. Third, this study was conducted in three institutions but surgical implants and perioperative cares had not been controlled, which might lead to clinical heterogeneity since PROs could be affected by these confounding factors. So a prospective study with more consistent protocols will preferably advocate the technical superiority. Furthermore, we had not measured subaxial alignments, which might interact with upper cervical reconstruction after surgery and jointly affect PROs.
CONCLUSION
Three-planar AAI should be reconstructed by C1 LMS-C2 PS fixation, while sagittal and coronal AAI could be corrected by C1 LMS-C2 TLS fixation. PROs could be improved after atlantoaxial reconstruction for patients with chronic AAI. C1–2 Cobb angle is an independent factor relates to improvement of PROs after correcting chronic AAI, so does the patient’s age ≤40 years to postoperative NDI. To extend the clinical application, both of PS fixation and TLS fixation could be applied to correct chronic AAI in selected patients. However, TLS fixation may replace PS fixation to treat AAI patients for avoiding some surgical complications and high-tech requirement.
Notes
The authors have nothing to disclose.
Acknowledgements
This study was financially supported by the grants of China Scholarship Council (2017-3109/201708260068) and 5511 Innovation-driven Program of Jiangxi Province Department of Science and Technology (20165BCB18017). We thank Sun Kyu Choi (Yonsei University College of Medicine) and Huiyong Hu (Children’s Hospital of Shanghai) for their statistical suggestions.