Immediate Revision Surgery due to Post-Anterior Cervical Discectomy and Fusion (ACDF) Spinal Epidural Hematoma
Article information
Abstract
Anterior cervical discectomy and fusion(ACDF) is a surgical treatment for cervical radiculopathy and myelopathy. Though this is a common surgery, spinal epidural hematomas occur rarely and an immediate treatment decision and surgical decompression are required in this situation. In this report, we discuss the proper treatment of spinal epidural hematoma after ACDF.
INTRODUCTION
The anterior cervical spinal approach is commonly used for the surgical treatment of disc herniation, spinal lesions caused by osteoarthritis, and fractures or joint dislocations of the cervical spine3). The incidence of complications associated with this type of surgery is low2,7,9). Though this is a common surgery, post-operative complications should not be overlooked. Neural injury, hoarseness, wound infection, CSF leakage, and post-op hematomas can all develop after ACDF.
Neural injury causing neurological deficits can be fatal to patients. Direct neural injury during the actual surgery is rare, but even an experienced surgeon can be challenged when confronted with neurological deficits that develop after surgery caused by an unexpected post-operative hematoma. In this report, we introduce the proper treatment for an epidural hematoma after ACDF.
CASE REPORT
A 36-year-old male patient who worked as a welder received physiotherapy for right shoulder pain and right C6 dermatomal radiating pain over a period of three months. However, there was no improvement with conservative treatment. On neurological examination, Spurling sign and Lhemitte's sign were positive, and right triceps weakness was noted as grade IV(Fig. 1). A degenerative herniated cervical disc was seen on the right side of C6/7, and ACDF was subsequently performed on the C6/7 segment using a Solis cage on May 25, 2009. The total surgery time was 108 minutes, and estimated blood loss was 50 cc. After surgery, the patient was transferred to the recovery room and showed no neurologic deficits.

Pre-op MRI. A herniated cervical disc at C6/7 (Rt) was seen on T2 weighted sagittal and axial pre-op MRI.
In the recovery room, the patient complained of a sudden headache, and his systolic blood pressure immediately rose to 200mmHg, although he has no any medical problem. Five minutes later, he developed grade 2 and grade 1 quadriaresis of the upper and lower extremities, respectively. Hypoesthesia also developed below the T2 level. A magnetic resonance imaging (MRI) was performed within 30minutes after the onset of symptoms. An extended epidural hematoma was revealed from C2 to T5, ventral to the spinal cord, on the immediate post-op MRI (Fig. 2).

Immediate post-op MRI. Ventral epidural hematoma extending from C2-T5 was noted on the T2 weighted sagittal MRI acquired immediately after ACDF using a Solis cage on C6/7 was performed.
He was transferred to the operating room again and underwent an immediate revision operation. Fresh blood was evacuated once the cage was removed, and the compressed ventral dura was decompressed. We could not find an active source of bleeding in the operating field, so we repositioned the cage again after complete hemostasis was achieved and then inserted a hemovac tube (Barovac SS200M, ID 1.6mm, OD 3.2 mm) before finishing the surgery.
On neurological exam after the revision ACDF, upper and lower extremity motor weakness had recovered to grade 4+, and the hypoesthesia below T2 had slightly improved (Fig. 3). At the three-month post-op follow-up visit the patient had a completely normal neurologic examination, except he complained of mild urination difficulties at night. The post-op epidural hematoma had completely disappeared on follow-up imaging (Fig. 4). His neurologic symptoms were completely normal at his six-month post-op follow-up visit.
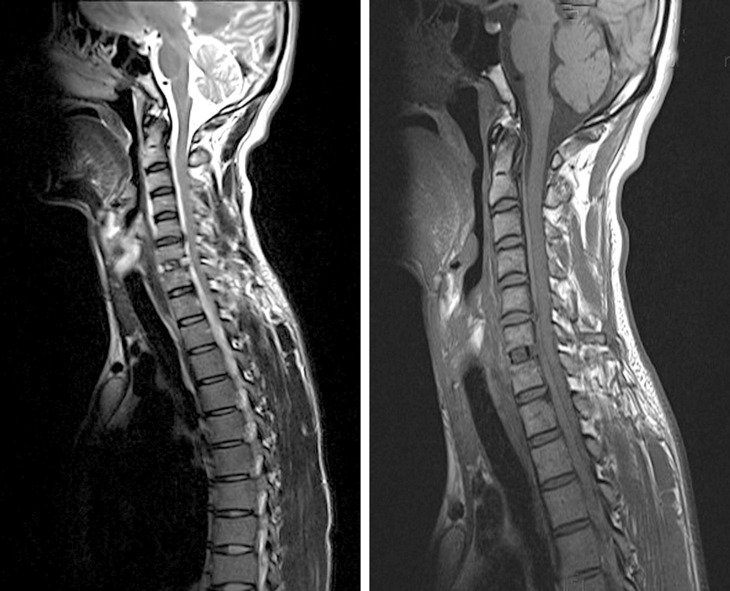
T2 and T1 weighted sagittal MRI acquired immediately post-revision. Spinal cord decompression was performed, but a residual epidural hematoma remained from C2-T5.

T2 and T1 weighted sagittal MRI taken three months postoperatively. No residual epidural hematoma was seen.
DISCUSSION
Causes of spinal epidural hematomas include trauma, indwelling spinal catheters, anticoagulation therapy, lumbar puncture, blood dyscrasias, infections, vascular malformations, pregnancy, and spine surgery1,4). The incidence of post-operative spinal epidural hematomas is very low at 0.24%1,5,8). When a spinal epidural hematoma leads to neurological deficits, imme diate and proper active treatment is required. Post-op epidural hematomas can be challenging for even the most experienced surgeon.
In this case, the patient underwent a MRI within 30minutes after the onset of quadriparesis, and all necessary procedures, including immediate revision surgery, were performed within one hour. Prompt examination and active surgical treatment prevented the patient's neurologic deterioration.
A surgical approach is the key to managing this condition. In this case, a ventral longitudinal epidural hematoma extending from C2 to T5 was discovered, which included the operative wound. For decompression of all involved areas, we considered decompressive laminectomy through a posterior approach with hematoma removal. However, we also considered an immediate one level hematoma evacuation from the most severely compressed area of the spinal cord by the anterior approach through the original surgical incision. In this case, despite the extensive epidural hematoma, we conducted hematoma evacuation and achieved hemostasis through the original surgical incision, and the remaining hematoma resolved with time. Removal of the loculated hematoma at the index level was sufficient to relieve the patient's neurological symptoms6). In addition, the anterior approach was feasible because it was an immediate revision. Hematoma removal and decompression is more likely to be difficult if delayed; therefore, when this kind of epidural hematoma is detected, it is important to re-approach the original surgical site for removal and decompression of the hematoma.
To prevent post-ACDF epidural hematomas, bleeding control is very important. This procedure is different from brain surgery, as dura tenting suturing cannot be performed in spine surgery. Thus, when carrying out this procedure, dura detachment should be minimized, and posterior longitudinal ligament (PLL) should be preserved if PLL elimination is not necessary. In addition, it is better not to pack material such as Gelform densely around the cage because it could plug the hematoma in the epidural space behind the disc space.
CONCLUSION
Although post-ACDF spinal epidural hematomas are rare, they can be fatal for the patient. If a hematoma is suspected, prompt radiological evaluation, diagnosis, and immediate anterior revision surgery without delay is essential.