Surgical Impact on Global Sagittal Alignment and Health-Related Quality of Life Following Cervical Kyphosis Correction Surgery: Systematic Review
Article information

Abstract
When spinal imbalance occurs, the human body reacts through various compensatory mechanisms to maintain the head over the pelvis and to retain a horizontal gaze. These compensations occur through mobile spine segments as well as pelvic tilt and lower extremities. The purpose of this review was to understand the surgical impact on global sagittal alignment and health-related quality of life (HRQoL) following cervical kyphosis correction surgery. The cervical kyphosis correction surgery induces reciprocal changes in craniocervical and thoracolumbar alignment. Successful cervical deformity correction needs to focus not only on restoring proper cervical lordosis, but also on achieving global balance of the cervical spine with other parts of the spine. The goal of the surgery is to achieve occiputtrunk (OT) concordance (the center of gravity-C7 sagittal vertical axis < 30 mm) and cervical sagittal balance. Once OT-concordance is achieved, subsequent thoracolumbar alignment changes occur as needed to harmonize global spinal alignment. Reciprocal changes after surgery exhibit different patterns depending on whether patients have compensation ability in their thoracolumbar spine or not. C2–7 sagittal vertical axis and sagittal morphotype of the cervical kyphosis are correlated with HRQoL. Changes in cervical lordosis minus T1 slope correlate to HRQoL improvements.
INTRODUCTION
When spinal imbalance occurs, the human body reacts through various compensatory mechanisms to maintain an erect posture, with the head over the pelvis, and to retain a horizontal gaze [1-3]. A single change in one segment induces a change in the reciprocal segment due to the flexibility of the spine. These changes occur not only through mobile spine segments, but also pelvis and the lower extremities [4]. In primary thoracolumbar deformities, the loss of lumbar lordosis (LL) is accompanied by an increased pelvic tilt (PT), cervical hyperlordosis, hip extension, knee flexion, and ankle dorsiflexion [5]. Similarly, primary cervical deformities contribute to thoracolumbar deformities and spinopelvic imbalance [2,6]. Cervical sagittal imbalance causes significant impairment due to the inability to gaze horizontally and is associated with poorer health-related quality of life (HRQoL) and functional disability [2,7,8]. Compensation in primary cervical kyphosis occurs via posterior shifting of C7 sagittal vertical axis (SVA) (distance between C7 plumb line (PL) and posterosuperior corner of the S1 endplate), a small T1 slope (TS), and large LL.
Surgical correction of cervical kyphosis can result in compensatory changes in spinal alignment beyond the fused spinal segment, which are termed reciprocal changes [4]. Only a few authors have analyzed the surgical impact on global sagittal alignment (GSA) and HRQoL following cervical kyphosis correction surgery [7,9-11]. No systematic review article on this topic has yet been published. This study was designed to provide an overview of reciprocal global skeletal changes and clinical impact by HRQoL after cervical kyphosis correction surgery.
MATERIALS AND METHODS
We carried out a search of PubMed, Embase, and Cochrane Library for studies published through May 2020, using “cervical surgery,” “sagittal alignment,” “change,” and “HRQoL” as search terms. Case reports and articles that did not focus on reciprocal changes in GSA after cervical kyphosis correction surgery were excluded. Eight articles were ultimately included in this systematic review (Table 1).

Summary of the articles included in this systematic review
1. Alignment of Normal Cervical Spine
Traditional teaching describes normal cervical alignment as being lordotic due to anteroposterior height difference of the intervertebral disc and vertebral body. Previously, loss of cervical lordosis (CL) has been believed as a pathological cause [12,13]. Hey et al. [14] studied physiological alignment of the cervical spine using EOS system (EOS Imaging, Paris, France). In contrary to normal LL due to sacral slope, normal cervical alignment is not necessarily lordotic [12]. It is as a result of the cervical alignment affected by not only TS, but also other many variable parameters [15]. The authors found that 73.0% of healthy human do not have CL upon standing. Another study has shown that cervical kyphosis is present in up to 34% of asymptomatic people [16]. TS and C7 SVA are most significantly correlated with the CL. Low TS and negative C7 SVA could induce physiological kyphosis of the cervical spine. Therefore, routine lordotic correction of the cervical spine may not necessarily be helpful in certain patients. The cervical sagittal alignment can be varied depending on the postures. Greater CL occurs in the sitting posture due to an increase in TS and C7 SVA.
2. Assessment of Cervical Spine Deformity
The etiology of cervical kyphosis is variable and while the most common etiology is iatrogenic. Other causes include disc degeneration, systemic inflammatory disease, congenital, oncologic and pathologic causes [17]. In comparison with thoracolumbar deformity, there was a limited understanding of the most important clinical and radiographic parameters for patients with cervical spinal deformity (CSD). Ames et al. [2] made meaningful attempt to create a comprehensive classification of CSD using modified version of the Delphi approach. Hyun et al. [7] suggested a revised version of the classification using long-term follow-up data (Fig. 1). This classification consists of deformity descriptor with 5 modifiers and provides mechanism to assess CSD with a perspective of GSA. Deformity descriptor provides grouping of the deformity type by the location of the deformity apex. The 5 modifiers consist of C2–7 SVA (distance between C2 PL and C7 PL), horizontal gaze, TS–CL, myelopathy, and the Scoliosis Research Society (SRS)-Schwab classification. First, C2–7 SVA is correlated with Short-Form-36 physical component and Neck Disability Index (NDI) scores negatively and positively, respectively. Second, for horizontal gaze, a chin-brow to vertical angle (CBVA) is a measure of horizontal gaze. This parameter has been associated with favorable outcomes following correction of spinal deformity, including improved horizontal gaze, ambulation, and activities of daily living [18]. The CBVA of 10° has been described as an optimal target. Third, for TS–CL, the relationship between CL and TS is similar to the relationship between LL and PI [19]. Large TS induces large CL to balance the head over the pelvis as like large PI induces large LL for balanced alignment. Fourth, development of myelopathy has been associated with progressive cervical kyphosis and positive sagittal cervical alignment [20]. The modified Japanese Orthopedic Association score is wide accepted quantitative functional assessment of the severity of spondylotic myelopathy, which is range from 0 to 18 with lower scores reflecting a more severe impact [21]. Fifth, the SRS-Schwab classification consists of 4 coronal curve types and 4 sagittal modifiers and is correlated with HRQoL [22]. Cervical deformities are contributed to thoracolumbar deformities. Positive sagittal spinopelvic malalignment induces compensatory mechanism with increased CL in an effort to maintain horizontal gaze [23]. Therefore, classification of CSD should be assessed not only isolation of cervical spine but also thoracolumbar and spinopelvic parameters. A full-length lateral radiograph including cervical spine and femoral head is needed to apply this classification system. Passias et al. [24] recently demonstrated the validity of the classification system by retrospective review of 84 patients. They demonstrated that CSD patients described using the classification reveals associations between cervical and thoracolumbar alignment and preand postoperative measures of patient disability.
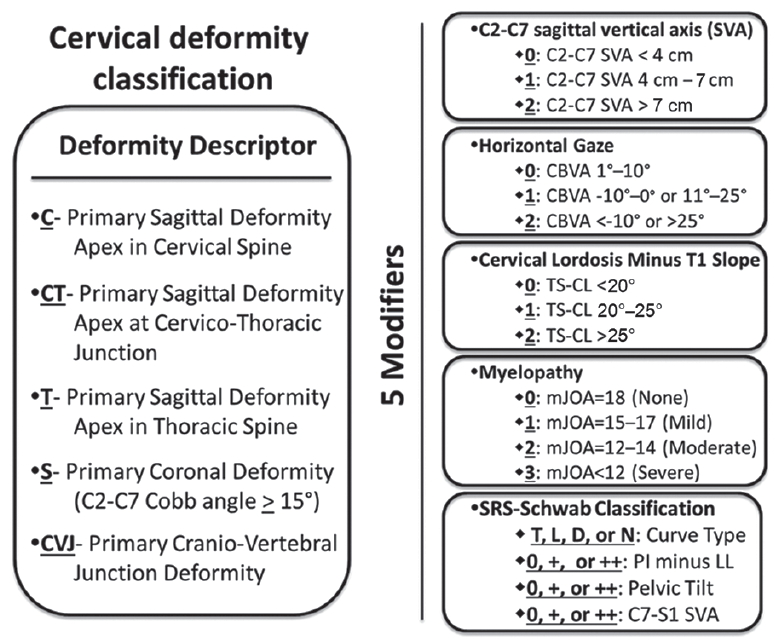
Revised cervical spinal deformity classification system [7], which consists of a deformity descriptor and 5 modifiers. CBVA, chin-brow to vertical angle; TS, T1 slope; CL, cervical lordosis; mJOA, modified Japanese Orthopedic Association score; SRS, Scoliosis Research Society; PI, pelvic incidence; LL, lumbar lordosis; D, double; L, lordosis; T, thoracic; N, none.
3. Surgical Impact on GSA Following Cervical Kyphosis Correction Surgery
Surgical indications of cervical kyphosis are either a severe kyphotic deformity on presentation, a progression of sagittal deformity, in conjunction with severe axial neck pain, neurological deficit, or functional disability [17,25]. Surgical approaches of the deformity correction include anterior, posterior, or combined anterior and posterior (360°) approach [26]. Not a few factors are considered to determine which of the approach is needed, including the location of compressive pathology, type, flexibility and location of the deformity [27,28].
There has been no clear goal of CL to be achieved in cervical deformity correction surgery. Similar to C7 SVA which is traditionally used to measure sagittal alignment of the thoracolumbar deformity, C2–7 SVA is acceptable in cervical deformity correction [29]. Compensation in primary cervical kyphosis occurs via posterior shifting of C7 SVA, small TS, and large LL [9,30]. TS, thoracic inlet angle, C2 PL, and CBVA are also increasingly being used [31]. To evaluate these parameters, a clinical whole skeletal image of the patients is needed [32]. Only a few studies have analyzed the compensatory mechanism of cervical kyphosis and reciprocal changes after cervical kyphosis correction surgery.
Miyamoto et al. [33] reported effect of cervical reconstruction surgery on compensatory mechanisms in GSA. They demonstrated that C0–1 angle (the angle between McRae’s line and the line passing through both the anterior tip of the anterior arch and the posterior tip of the posterior arch of the atlas) and clivo-axial angle (the angle between the line on the dorsal surface of the clivus and the line passing through the middle of the dens) are more important in the compensatory mechanism for kyphotic deformity at middle/lower cervical spine compared to downward parameters such as TS, LL, PI, and PT. To maintain a horizontal gaze, cranio-cervical junction lordosis increases with greater kyphosis at the middle/lower cervical spine. Correction of the middle/lower cervical spinal kyphosis results in normalization of the upper cervical spine due to no longer need for compensatory mechanism for maintaining horizontal gaze.
Mizutani et al. [10] described how cervical reconstruction surgery affects GSA changes. The goal of cervical kyphosis correction surgery is to achieve occiput-trunk (OT) concordance (the center of gravity-C7 SVA < 30 mm) and cervical sagittal balance. Once OT-concordance is achieved, subsequent thoracolumbar alignment changes occur as needed to harmonize the entire spinal alignment after surgery. They divided the 2 groups according to location of C7 PL (Fig. 2). Head-balanced kyphosis is a head position on the femoral head with posterior shifting C7 PL by compensatory changes of low angle of upper cervical spine and TS. Posterior shifting of C7 PL was made by hyperlordotic lumbar curve with larger LL than PI and thoracic hypokyphosis. Trunk-balanced kyphosis is anterior shifting of center of gravity PL with C7 PL located on the femoral head. These patients have a large TS, hyperlordotic upper cervical angle, and upper limit of PI–LL harmonization. There are significant different reciprocal changes after surgery between the 2 groups. In the head-balanced kyphosis, C7 PL moves anterior and subsequent TS, thoracic curve increase while LL decreases following surgery (Fig. 3). These restorations following the surgery achieve better GSA. In the trunk-balanced kyphosis, TS and thoracic kyphosis decrease and the head moves posteriorly following surgery. There are no significant changes in thoracolumbar alignment in the trunk-balanced kyphosis (Fig. 4).

Compensation mechanisms in patients with symptomatic primary cervical kyphosis. PL, plumb line; CK, cervical kyphosis; LL, lumbar lordosis; PI, pelvic incidence; TK, thoracic kyphosis.

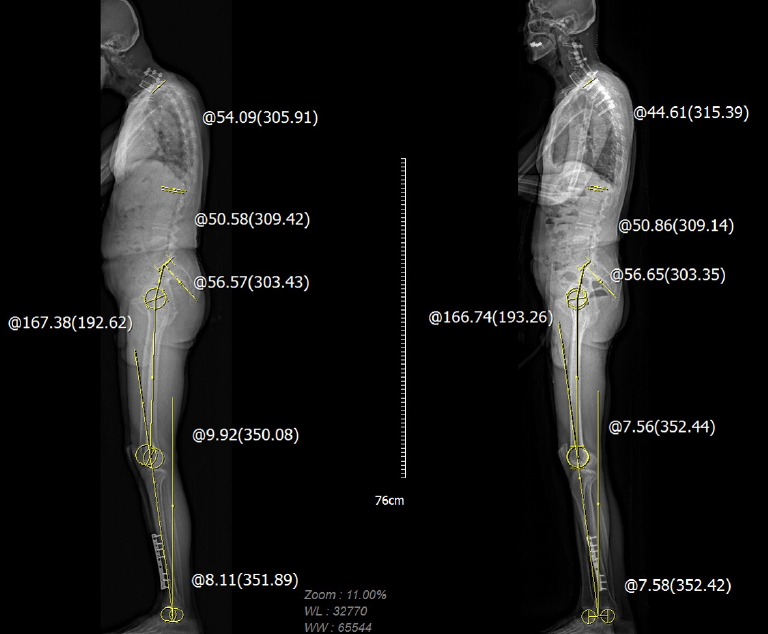
A representative case of a patient having compensated cervical kyphosis. Pre- (A) and postoperative whole-body EOS lateral image (B) showing that center of gravity (COG) plumb line (PL, blue line) was located on the femoral head, but the C7 PL (red line) was located markedly posteriorly. Cervical malalignment was corrected to achieve global sagittal balance (sagittal vertical axis [SVA]C2, SVACOG–C7 and SVAC2–7 & 40 mm) and OT concordance (distance between the COG PL and C7 PL & 30 mm). TK, thoracic kyphosis; LL, lumbar lordosis; PI, pelvic incidence; SRS, Scoliosis Research Society; SF-36 PCS, Short-Form-36 physical component; NDI, Neck Disability Index; ODI, Oswestry Disability Index; VAS, visual analogue scale; SFA, sacrofemoral angle; KA, knee angle; AA, ankle angle.
Whole-body images of a patient having decompensated cervical kyphosis. T1 slope and throracic kyphosis decreased while spinopelvic- and lower extremity parameters did not change following cervical deformity correction surgery.
We suggest that the reciprocal changes after cervical kyphosis correction surgery exhibit different patterns depending on whether patients have compensation ability in their thoracolumbar spine or not. Thus, in our clinical practice, we divide a compensated- and decompensated cervical kyphosis subgroup. In the compensated cervical kyphosis, preoperative posterior shifted C7 PL moves anteriorly after surgery, and subsequently thoracic curve and TS increase while lumbar hyperlordosis decreases. There are no significant changes in thoracolumbar alignment in the patients having decompensated cervical kyphosis following surgery. While TS and thoracic kyphosis decrease, spinopelvic and lower extremity parameters do not change after surgery. Furthermore, we found that pelvic- and lower extremity parameters do not change after kyphosis correction in the both groups.
4. HRQoL Related to Cervical Kyphosis
Sagittal imbalance of the thoracolumbar spine has been related to disability and unfavorable HRQoL in previous studies [34,35]. Sagittal imbalance can induce increasing energy expenditure and develop painful compensatory alignment changes [36-38]. There have been some studies about HRQoL related to sagittal malalignment in spinal deformity or related to thoracolumbar or spinopelvic imbalance [35,39-41]. In despite of commonly performed multilevel cervical fusion surgery, only a few authors have analyzed HRQoL after cervical kyphosis correction surgery.
Tang et al. [11] demonstrated that the severity of disability increases with positive sagittal malalignment following surgical reconstruction. They found positive correlation between C2–7 SVA greater than 40 mm and NDI score. C1–2 lordosis constitutes almost 80% of total CL. C1–2 alignment acts as the terminal link between the cranium and the cervical spine to maintain the horizontal gaze [42]. C2–7 SVA was strongly correlated with C1–2 lordosis. These relationships indicate that positive sagittal malalignment requires more energy expenditure to maintain the horizontal gaze and it induces adverse effect on HRQoL. Hyun et al. [7] assessed the sagittal alignment of cervical spine and HRQoL. They found significant correlations between C2–7 SVA and NDI scores which were similar to previous study. Furthermore, they demonstrated TS–CL correlated positively with C2–7 SVA, NDI scores and suggested a revised CSD classification system. Passias et al. [43] demonstrated myelopathy improvement as a key driver of patient outcomes following surgery.
Virk et al. [44] evaluated radiographic characteristics of CSD patients who achieved optimal HRQoL following reconstruction surgery. They divided cervical deformity patients into 3 groups: focal deformity, flat neck (TS–CL and lack of compensation), and cervicothoracic group. Within focal deformity group, maximal kyphosis correction correlated with better outcome. Flat neck patients with HRQoL improvement showed greater postoperative correction of the horizontal gaze. Cervicothoracic patients with HRQoL improvement had balanced global alignment both pre- and postoperatively. They concluded that the recognition of the sagittal morphotype of the deformity and distinct intraoperative goals including proper sagittal global/cervical alignment can help surgeons for achieving better outcomes.
Although a few studies have been reported HRQoL following cervical kyphosis correction surgeries, there were some studies about HRQoL after cervical surgery for not deformity or thoracolumbar deformity patients. Passias et al. [45] compared 2-year follow-up postoperative HRQoL among cervical only, thoracolumbar only, and combined deformity patients. They demonstrated that cervical deformity patients were more likely to better HRQoL within the early postoperative period and greater state of postoperative back pain for longer amount of time compared with other deformities. After 2-year follow-up, all deformity types showed similar HRQoL improvement. Tang et al. [11] found a significant correlation between a high C2–7 SVA and worse HRQoL after posterior cervical fusion surgery.
DISCUSSION
Cervical kyphosis can be debilitating to the patient, as well as challenging to the spine surgeon [17]. This study was designed to provide comprehensive background materials for compensatory mechanism of whole skeletal change of cervical kyphosis and to emphasize the impact on GSA and HRQoL after cervical reconstructive surgery. The cervical sagittal alignment ranges from lordosis to kyphosis. This could be a result of primary cervical pathology or compensatory change following thoracolumbar deformities. Many surgeons have been strived to restore CL, which showed that symptomatic healthy individuals have non-lordotic cervical spine. They generate CL may not always necessarily be physiological or ideal [14]. Whole skeletal alignment evaluation is necessary to differentiate these causes and to correct the primary cervical kyphosis.
Primary cervical kyphosis has different compensatory changes and postoperative reciprocal changes according to compensation ability in the thoracolumbar spine. Successful CSD correction needs to focus not only on restoring proper CL, but also on achieving global balance of the cervical spine with other parts of the spine [28]. The goal of surgery would be to achieve OT-concordance and cervical sagittal balance. Center of gravity of the head PL and C7 PL move onto the femoral head as needed to achieve OT-concordance [34]. There is increasing interesting in whole skeletal alignment before- and after deformity surgery. Recently, some spine surgeons studied reciprocal cervical changes following thoracolumbar deformities surgery. Patients with thoracolumbar malalignment exhibit compensatory changes with cervical hyperlordosis, pelvic shift, knee flexion, and hip extension. Ha et al. [46] studied 49 patients undergoing thoracolumbar spine surgery and demonstrated that preoperative C7 SVA affects postoperative reciprocal change of cervical spine. They found that preoperative low C7 SVA group (C7 SVA ≤ 6 cm) tend to have hypolordotic cervical curve and increase CL following surgery, while high C7 SVA group (C7 SVA ≥ 9 cm) have high CL preoperatively and decrease CL following surgery. Studies about reciprocal change of GSA and HRQoL following primary cervical kyphosis correction surgery are insufficient. More prospective or retrospective studies of large population are needed.
CONCLUSION
Compensation in primary cervical kyphosis is via posterior shifting of C7 SVA, small TS, and large LL. These compensatory mechanisms resolve reciprocally in a different fashion following cervical correction surgery according to compensation ability in the thoracolumbar spine. The goal of cervical reconstruction surgery would be to achieve sagittal balance regarding position of the head and GSA including the pelvis and lower extremities.
Notes
The authors have nothing to disclose.