Perioperative Outcomes in 17,947 Patients Undergoing 2-Level Anterior Cervical Discectomy and Fusion Versus 1-Level Anterior Cervical Corpectomy for Treatment of Cervical Degenerative Conditions: A Propensity Score Matched National Surgical Quality Improvement Program Analysis
Article information

Abstract
Objective
To compare the perioperative morbidity of 2-level anterior cervical discectomy and fusion (ACDF) with that of 1-level anterior cervical corpectomy and fusion (ACCF) for the treatment of cervical degenerative conditions.
Methods
A retrospective study of the 2005–2016 National Surgical Quality Improvement Program database for patients undergoing 2-level ACDF and 1-level ACCF was performed. Patient data included: age, sex, body mass index (BMI), functional status, and American Society of Anesthesiologists (ASA) physical status (PS) classification. Hospital data included: operative time and length of hospital stay (LOS). Thirty-day outcome data included: any, serious, and minor adverse events, return to the operating room, readmission, and mortality. After propensity matching for age, sex, ASA PS classification, functional status, and BMI, multivariate logistic regression analysis was used to compare outcomes between the 2 propensity-matched subcohorts. Finally, multivariate logistic regression that additionally controlled for operative time was performed to compare the 2 propensity-matched subcohorts.
Results
A total of 17,497 cases were identified, with 90.20% undergoing 2-level ACDF and 9.80% undergoing 1-level ACCF. Patients undergoing 2-level ACDF were younger, more likely to be female, had higher functional status, and had shorter operative time and LOS (p < 0.001). After propensity score matching, cases undergoing 1-level ACCF had a statistically significant higher rate of serious adverse events (p = 0.005). This difference was no longer significant after controlling for operative time.
Conclusion
While there was noted to be additional morbidity in 1-level ACCF cases relative to 2-level ACDF cases, the lack of difference once controlling for the surgical time supports using the procedure that best accomplishes the surgical objectives.
INTRODUCTION
Cervical spondylosis is a common cause of neurologic symptoms related to the cervical spine. Spondylosis leading to cervical radiculopathy and cervical myelopathy can significantly impair the quality of life of affected patients [1-3]. Compared to nonoperative management of symptomatic moderate to severe cervical spondylosis, surgical treatment has been shown to result in improved functional status, decreased pain, and better overall patient prognosis [4-7]. In fact, cervical spondylosis remains one of the most common disorders treated by spine surgeons with a nearly 7-fold increase in the number of cervical fusions performed in recent years [8].
The anterior approach to the cervical spine, first described in the late-1950s [9,10], is effective at removing ventral compression of the cervical spinal cord and cervical nerve roots, such as herniated disc material and osteophytes. This approach allows direct decompression of the neural elements with an opportunity to restore interbody height, improve cervical lordosis, and stabilize affected cervical spine segments [11].
Two-level anterior cervical discectomy and fusion (ACDF) is a common surgical treatment for 2-level cervical pathology [12]. However, 1-level anterior cervical corpectomy and fusion (ACCF) may also be considered to address 2-level cervical stenosis [13-18]. ACCF is generally selected to address retro-vertebral stenosis or cord compression. Some have suggested that the 2 healing surfaces of ACCF may be more easily fused than the 4 healing surfaces of a 2-level ACDF, although this remains a topic of debate [19].
Both 2-level ACDF and 1-level ACCF have been performed for decades and long-term results have shown that both procedures improve symptoms related to cervical radiculopathy and cervical myelopathy [20-22]. In certain clinical situations, the treating spine surgeon may consider either 2-level ACDF versus 1-level ACCF. In these situations, it is not clear if there is a different perioperative morbidity profile for these procedures.
The current study was designed to take advantage of the high data quality and large sample size afforded by the American College of Surgeons National Quality Improvement Program (NSQIP) database to examine the demographics, comorbidities, and perioperative complications in matched patients undergoing 2-level ACDF versus 1-level ACCF in a large, national study population.
MATERIALS AND METHODS
1. Data Source
NSQIP collects over 250 variables from representative surgical cases performed at more than 600 participating institutions across the United States. Interrater discordance has been shown to be less than 1.5% due to vigorous data collection and audit protocols mandated by NSQIP. Our Institutional Review Board exempted this study from further consideration.
2. Study Cohort
Patients who underwent 2-level ACDF or 1-level ACCF were included in the study population. Cases of ACDF were identified using Current Procedural Terminology (CPT) codes 22551, 22554, and 63075. Additional levels of ACDF were identified by counting the number of instances of the CPT code 22552, 22554, and 63076. ACDF cases that included more than one “additional level” codes (indicating more than 2 operative levels) were excluded from the study population. Patients who had a corpectomy in addition to 2-level ACDF were excluded from analysis. Patients who underwent ACCF were identified using CPT code 63081. Cases that involved more than 1-level corpectomy were excluded from the study population (those with CPT codes 63082 or 22846). Patients who underwent ACDF in addition to corpectomy were further excluded.
Patients who underwent concomitant posterior cervical procedures (i.e., cervical laminectomy, posterior cervical fusion, cervical laminoplasty) were excluded from analysis. Cases involving neoplasms, trauma, and infection were identified using diagnostic codes and were further excluded from the study population.
Patient demographic characteristics including age, sex, height, and weight were extracted from the NSQIP database. Body mass index (BMI) was calculated from height and weight data. Preoperative functional status and American Society of Anesthesiologists (ASA) physical status (PS) classification were directly recorded from the NSQIP database. ASA PS classification has been shown to reliably approximate the patient’s comorbidity burden prior to operation. Operative time (in minutes) and length of hospital stay (LOS, in days) were extracted from NSQIP.
3. Postoperative Adverse Outcomes
NSQIP records the occurrence of postoperative adverse outcomes, regardless of discharge status, for 30 days following operation. The occurrence of these individual complications was extracted from the database and binned into 3 complication categories: any adverse events (AAEs), serious adverse events (SAEs), and minor adverse events (MAEs).
A SAE was defined as the occurrence of any of the following: deep surgical site infection, sepsis, failure to wean, unplanned reintubation, postoperative renal failure, deep vein thrombosis, pulmonary embolism, cardiac arrest, myocardial infarction, or stroke. A MAE was defined as the occurrence of any of the following: superficial surgical site infection, wound dehiscence, pneumonia, urinary tract infection, or postoperative renal insufficiency. The occurrence of AAE was defined as the occurrence of a major adverse event or MAE.
NSQIP began recording the number of 30-day readmissions for each case after the year 2011 and the number of 30-day reoperations for each case after the year 2012.
4. Statistical Analysis
Two-level ACDF and 1-level ACCF cohorts were first compared on the basis of patient demographic characteristics, operation time, and LOS. Categorical variables were compared using chi-square tests. Continuous variables were compared using Student t-tests and analysis of variance. The level of significance for tests of difference in demographic characteristics was set at 0.01 after Bonferroni correction for 5 hypotheses. The level of significance for tests of difference in operation time and LOS was set at 0.025 after Bonferroni correction for 2 hypotheses.
To account for differences in patient demographic characteristics and comorbidity burden between the ACDF and ACCF surgery cohorts, propensity score matching with a caliper width of 0.001 was performed to match patients based on age, sex, BMI, functional status, and ASA PS classification. This is a common statistical technique to account for potential nonrandom assignment of cases to ACDF or ACCF. The algorithm dropped 8 cases from the ACCF cohort that did not have a close enough match in the ACDF cohort. Ultimately, 2 new ACDF and ACCF cohorts were generated that had nearly identical patient demographic characteristics.
Multivariate logistic regression was then performed comparing the cohort while controlling for age, sex, BMI, functional status, and ASA PS classification. Odds of experiencing an adverse event in the ACCF group were determined, using the 2-level ACDF group as a baseline. Prior studies have shown that this statistical method, known as double adjustment matching, can be effective in removing residual bias after propensity score matching [23,24]. Next, because mean operative times continued to be statistically different after propensity score matching, a multivariate logistic regression that additionally controlled for operative time was performed for the propensity-matched cohorts. The level of significance for the aforementioned logistic regressions was set at p < 0.008, after Bonferroni correction to account for the 6 hypotheses being tested.
All statistical analyses were performed using Stata 13 (StataCorp LP, College Station, TX, USA).
RESULTS
1. Study Population
A total of 17,497 patients were identified for analysis based on the inclusion/exclusion criteria defined. Of these cases, 15,783 (90.20%) had undergone 2-level ACDF and 1,714 (9.80%) had undergone 1-level ACCF (Fig. 1). The analysis of readmission included 16,726 of 17,497 cases and the analysis of reoperation included 15,529 of 17,497 cases. These represent 95.6% and 88.7% of total cases respectively.
Number of cases by procedure. ACDF, anterior cervical discectomy and fusion; ACCF, anterior cervical corpectomy and fusion.
Patient characteristics are shown in Table 1. Patients who underwent 2-level ACDF tended to be slightly younger (mean age of 54.9 years in the ACDF cohort vs. 56.7 years in the ACCF cohort, p < 0.001), be more functionally independent (98.62% in the ACDF cohort vs. 94.81% in the ACCF cohort, p < 0.001), and have a lower average ASA PS classification (mean ASA of 2.4 in the ACDF cohort vs. ASA of 2.5 in the corpectomy cohort, p < 0.001). Therefore, propensity score matching was used to control for these potential confounding factors. Once matched, there were no longer significant differences in patient demographics or comorbidities (p > 0.900 for all).

Demographic and comorbid characteristics of patients who underwent 2-level ACDF vs. 1-level ACCF (n=17,497)
Patients who underwent 2-level ACDF had significantly shorter operative time than patients undergoing 1-level ACCF (140.7±66.1 minutes for the ACDF group compared to average of 172.1 ± 86.4 minutes [mean ± standard deviation] for the ACCF group; p < 0.001). The 2-level ACDF group also had shorter LOS than patients undergoing 1-level ACCF (1.9±6.7 days for the ACDF cohort vs. average of 3.6±10.5 days for the ACCF cohort; p < 0.001) (Table 2). After propensity score matching, cases of 2-level ACDF continued to have significant shorter operative time and LOS compared to 1-level ACCF cases (Table 2).

Operative time and total length of hospital stay of all patients by procedure type (n=17,497)
Perioperative outcomes (AAE, SAE, MAE, return to the operating room, readmission, and mortality) were assessed. The number of patients and percent patients experiencing these outcomes are listed in the left half of Table 3.
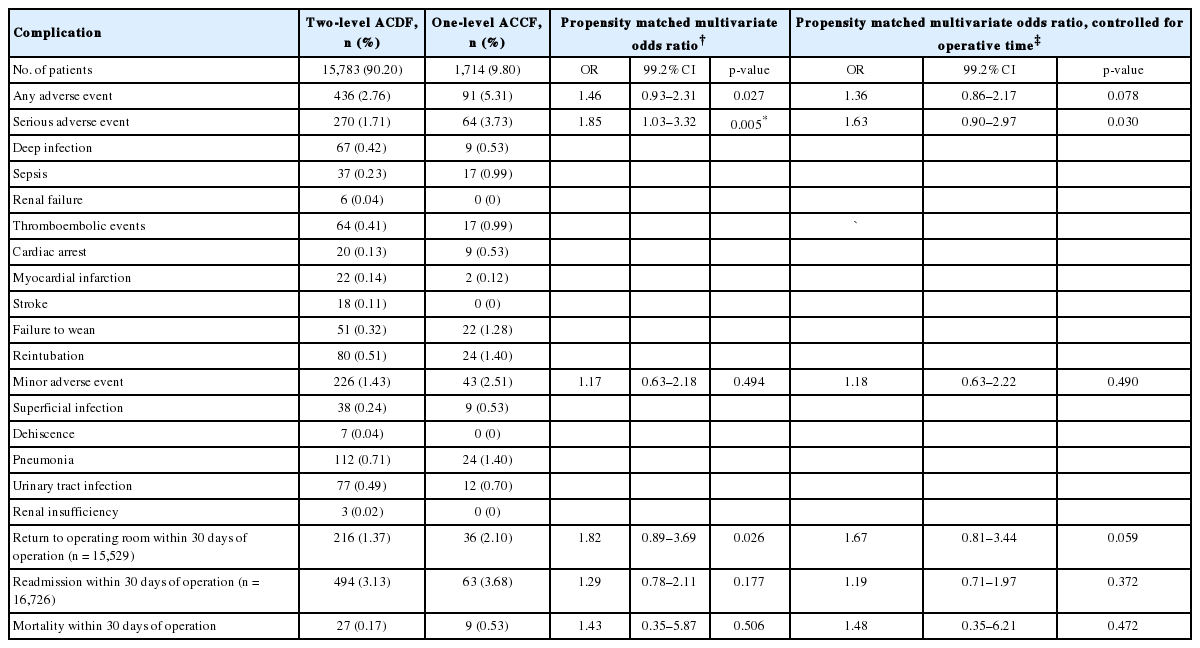
Number of adverse events, return to operating room, readmissions, and mortality for patients who underwent 2-level ACDF vs. 1-level ACCF (n=17,497)
2. Multivariate Regression on Propensity Score Matched Cohorts, Without Controlling for Operative Time
After propensity score matching, multivariate logistic regression models controlling for patient demographic factors and preoperative comorbidity burden were fitted on to the surgical outcomes of ACCF and ACDF cases. Patients who underwent 1-level ACCF compared to 2-level ACDF had increased odds of SAE (odds ratio, 1.85; 99.2% CI, 1.03–3.32; p = 0.005). There were no differences in the odds of AAE, MAE, reoperation within 30 days of index procedure, readmission within 30 days of index procedure, or mortality between patients undergoing 1-level ACCF versus 2-level ACDF (p > 0.008 for all) (Table 3).
3. Multivariate Regression on Propensity Score Matched Cohorts, Controlling for Operative Time
Multivariate logistic regression additionally controlling for operative time was then performed. After controlling for operative time, cases of 1-level ACCF did not have statistically significant increased odds of SAE. There continued to be no difference in the odds of AAE, MAE, reoperation, readmission, or mortality. These results are shown in Table 3 and Fig. 2.

Multivariate odds ratios for adverse events in patients who underwent 2-level anterior cervical discectomy and fusion (ACDF) versus 1-level anterior cervical corpectomy and fusion (ACCF). CI, confidence interval; BMI, body mass index; ASA, American Society of Anesthesiologists.
DISCUSSION
Two-level ACDF and 1-level ACCF may be considered for treatment of 2-level cervical stenosis. In fact, a recent study based on data from the American Board of Orthopaedic Surgery found that orthopaedic spine surgeons submitting board cases treated cervical pathology by anterior cervical approaches almost 90% of the time [12]. For 2-level disease, the surgical decision between 2-level ACDF and 1-level ACCF is often dictated by the pathology being addressed. However, there are clinical situations where pathology could be appropriately treated with either of these surgeries and the spine surgeon must decide between the 2 options.
The current study utilized 2005 to 2016 NSQIP data with a total of 17,497 patients, of which 90.20% underwent 2-level ACDF and 9.80% underwent 1-level ACCF for cervical degenerative pathology. Those undergoing 2-level ACDF were younger, more likely to be female, had a higher functional status and a lower mean ASA PS classification. These differences were addressed with propensity matching, after which there were no longer differences in demographics, functional status, or mean ASA PS classification.
After propensity-matched scoring and a performing a multivariate analysis controlling for patient factors, it was determined that patients undergoing 1-level ACCF have a significantly higher rate of SAEs, increased length of stay, and longer operative time than 2-level ACDF. When the multivariate analysis was repeated controlling for operative time, there was no difference in 30-day perioperative outcomes between the 2 surgical groups.
Previous studies comparing 2-level ACDF and 1-level ACCF have demonstrated similar clinical results between the 2 surgical procedures [25]. Oh et al. [26] published a retrospective series of 31 patients who underwent 2-level ACDF or 1-level ACCF with an average of 26-month follow-up. They found that operative time and bleeding were significantly greater in the corpectomy group, but that corpectomy patients had superior radiographic results (segmental height and cervical lordosis) compared with 2-level ACDF patients. The authors reported that both groups had similar pseudarthrosis rates and other clinical outcomes. Wang et al. [27] published a retrospective study of 52 patients who underwent 2-level ACDF or 1-level ACCF. This study found no significant difference in graft subsidence, pseudarthrosis, or clinical outcomes. Park et al. [28] performed a retrospective review of 97 2-level ACDF or 1-level ACCF patients. They found that graft subsidence and loss of cervical lordosis continued out further postoperatively for 1-level ACCF than 2-level ACDF, but that this was not associated with long-term clinical results or radiographic evaluation. Overall, these prior studies showed good clinical outcomes for both 2-level ACDF and 1-level ACCF. Limitations of the studies include relatively low patient numbers and the retrospective nature of the studies.
It is well established that 1-level ACCF is associated with longer length of stay and operative time than 2-level ACDF [29,30]. Song et al. [30] performed a retrospective review of 40 patients who underwent either ACDF or ACCF for multilevel cervical spondylotic myelopathy and had at least 5 years of postoperative follow-up. The authors found that both groups of patients had similar clinical outcomes as measured by visual analogue scale and Japanese Orthopaedic Association scores [30]. However, the ACDF group had shorter length of stay and operative times as well as lower blood loss [30]. Similarly, a meta-analysis performed by Guan et al. [29] included 13 randomized controlled studies and compared the outcomes of ACDF and ACCF in the treatment of cervical spondylotic myelopathy. These authors again found that the clinical outcomes were not statistically different but that ACCF patients had longer operative time and hospital stay as well as higher operative blood loss. In the currently presented study, the 1-level corpectomy group was found to have on average 30 additional minutes of operative time. Additionally, the average length of stay was 1 day in the ACDF group and 4 days for the corpectomy group. These findings are consistent with the results of the previous literature.
The limitations of this study mostly revolve around the database. NSQIP does not track spine specific variables. Thus, differences in morphological characteristics and surgical decisions making cannot be directly assessed. Furthermore, the present study is unable to ascertain whether 2-level procedures are performed at contiguous segments. In addition, the database does not track clinical or radiographic findings. Despite these limitations, the database is well suited to track medical and surgical perioperative adverse outcomes in the initial 30-day perioperative period, which is the time period in which patients undergoing anterior cervical surgery at the highest risk for a complication. Even with the inherent limitations present in all databases, the NSQIP database has been shown to have robust, validated data for the variables assessed [31-33].
Based on the results in the current study, 1-level ACCF has a higher rate of SAEs than 2-level ACDF, primarily driven by the longer operative time associated with 1-level ACCF. After controlling for operative time, there were no significant differences between the 2 groups. This data suggests that the surgeon should select the procedure that best accomplishes the surgical objectives required for a given patient’s pathology.
Notes
Dr. Jonathan Grauer has the following disclosures: Cervical Spine Research Society: Board or committee member Contemporary Spine Surgery: Editorial or governing board NASS Spine Line: Editorial or governing board North American Spine Society: Board or committee member TIDI Products: Paid consultant. The rest of our authors have nothing to disclose.
Acknowledgements
This study was supported by the National Institute on Aging of the National Institutes of Health under Award Number T35AG049685.