To the editor
We read with interest the article by Ohara et al. [1] titled “Full-Endoscopic Transcervical Ventral Decompression for Pathologies of Craniovertebral Junction: Case Series.” First, we would like to congratulate the authors. We believe that their new endoscopic approach is much safer and less invasive than the existing transoral and endonasal approaches to the craniocervical junction (CCJ) and upper cervical spine. However, the authors used a standard, Smith-Robinson anterior cervical approach; this may be inconvenient because the access is too lateral and too tangential to the upper cervical spine. The images clearly show that drilling proceeded at an angle of 30° to the anterior wall of C2. This highly tangential approach renders it difficult to drill the posterior-inferior body of C2. In our experience, the use of a standard, Smith-Robinson anterior cervical approach renders access above the C2–3 disc levels difficult. Resection is limited, particularly at the level of the odontoid tip, because of the trajectory. This is because the entry point is too low.
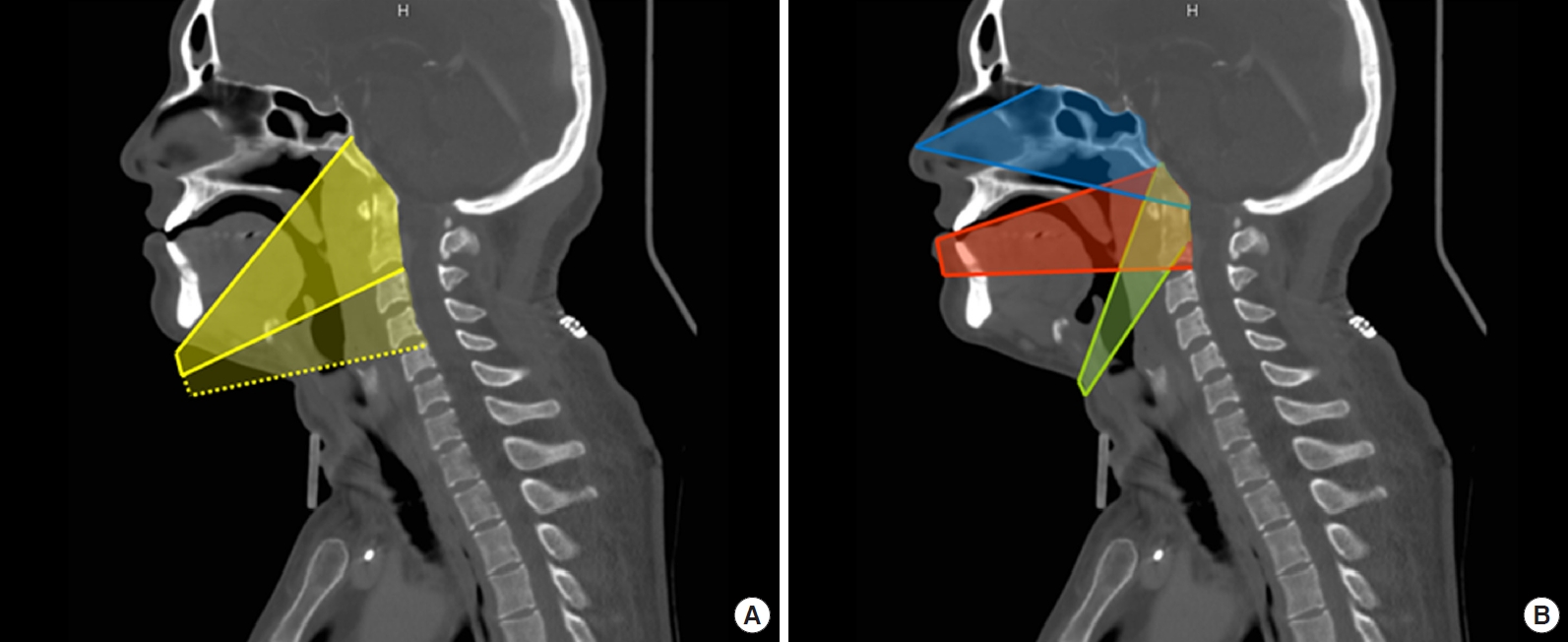
We strongly advise the use of an endoscopic, submandibular retropharyngeal approach [2]. A higher U-shaped incision arching 4–5 cm below the mandible would avoid injury to the marginal branch of the facial nerve. Next, the platysma muscle is rolled superiorly to expose the submandibular gland. At this stage, the surgeon can choose to pass under or go through that gland. If there is no need to go higher than the lower edge of C2, it is not necessary to resect the gland. However, if access to C2 or the anterior arch of C1 is required, we suggest resecting the submandibular gland to allow for maximum orthogonal access (Fig. 1), thus improving the quality of decompression.
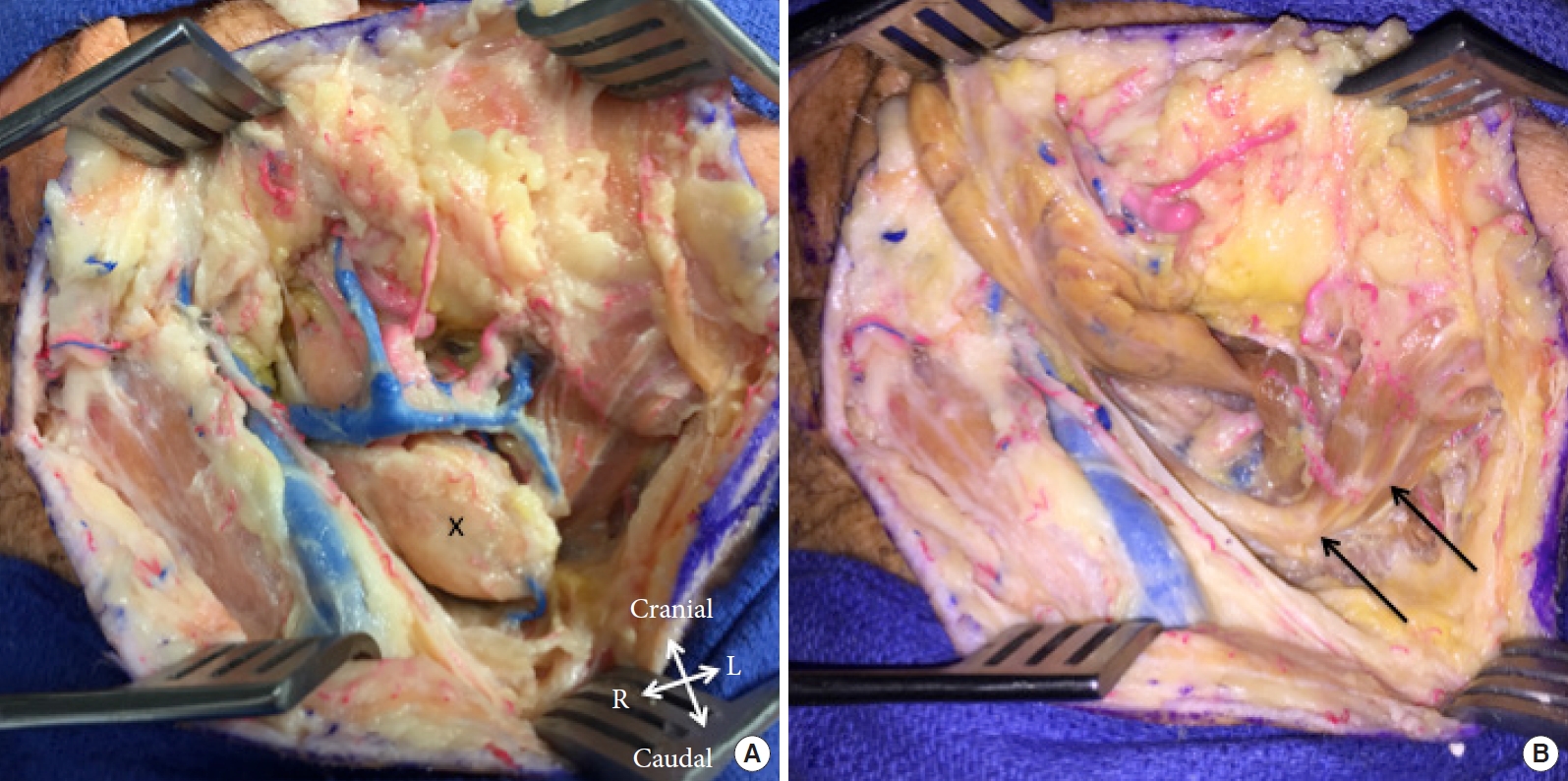
Once the submandibular gland has been removed, it is possible to observe a submandibular triangle formed by the lower edge of the mandible and the anterior and posterior bellies of the digastric muscle (joined at their apices by the digastric tendon) (Fig. 2). The hypoglossal nerve can be identified, and the mylohyoid muscle can be retracted anteriorly to allow direct access to the retropharyngeal space. This affords an orthogonal view centered on the C2–3 discs (Fig. 1).
Submandibular gland resection offers 2 principal advantages. The first is improved surgical exposure. The surgical corridor is completely changed, now being limited cranially by the mandible and caudally by the body of the digastric muscle. The operative field is considerably extended cranially, indeed up to the clivus, allowing orthogonal access to C2. Resection of C1 and the odontoid process are greatly facilitated, as is C1 plating. The second advantage is the decreased risk of hypoglossal nerve neuropraxia that can develop after prolonged retraction without gland resection.
This endoscopic, submandibular retropharyngeal approach is suitable when performing surgery on midline lesions that straddle the CCJ, such as the basilar invagination described by Ohara et al. [1]. Spinal surgeons may have to seek the assistance of ENT surgeons if the submandibular gland is to be removed. We strongly recommend the use of this approach when treating all midline lesions above the C2–3 disc.