Rehabilitation of Spinal Cord Injury: WFNS Spine Committee Recommendations
Article information

Abstract
Spinal cord injury (SCI) is accompanied by a significant number of complications associated with damage to the spinal cord, gross functional impairments leading to limited self-care and movement, leading to a high level of disability, social and psychological maladaptation of the patients. Besides, pain and spasticity negatively affect rehabilitation programs. This search was conducted in PubMed/MEDLINE database. All studies published in English language (n = 16,297) were considered for inclusion. Of all studies evaluating rehabilitation in SCI patients (n = 80) were included. Based on the literature review the faculty of the WFNS Spine Committee created statements covering different aspects of the contemporary rehabilitation process of the SCI patients. The prepared statements were subjected to discussions, followed by anonymous voting process by the members of the WFNS Spine Committee. As result of the diccussions and the voting process the statements were modified and published as recommendations of the WFNS Spine Committee. The care for the SCI has gone a long way from the times after the World War II when these patients were considered hopeless in terms of any functional recovery, to the contemporary comprehensive rehabilitation programs. The rehabilitation is important part of the modern comprehencive treatment of SCI patients nowadays. The current manuscript reflects different aspects of the contemporary rehabilitaton process and decision makings, which were discussed by the faculty of the WFNS Spine Committee resulting in issuing of the following recommendations.
INTRODUCTION
Spinal cord injury (SCI) is accompanied by a significant number of complications associated with damage to the spinal cord, gross functional impairments leading to limited self-care and movement, loss of control of the pelvic functions, and a high level of disability, social and psychological maladaptation of patients [1].
Disability as a result of damage to the spine and spinal cord varies from 57.5 to 96 and even 100%, amounting to 0.7% in the structure of the general contingent of disabled people [2].
In the recovery period of SCI effective rehabilitation is achieved through individual rehabilitation programs.
METHOD
This systematic review was carried out according to guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines. This search was conducted in PubMed/MEDLINE database. All studies published in English language (n = 16,297) were considered for inclusion.
The authors (NA, AK, EOF) independently identified the relevant studies based on the title and abstract. Subsequently, full text articles were screened for eligibility. All studies evaluating rehabilitation in SCI patients were included (n = 80). Exclusion criteria included any animal studies, case reports, or studies not published in the English language.
Based on the literature review the members of the World Federation of Neurosurgical Societies (WFNS) Spine Committee prepared statements covering different aspects of the contemporary rehabilitation process of the SCI patients. A presentation based on the literature review and the prepared statements were subjected to discussions, followed by anonymous voting process by the members of the WFNS Spine Committee (n = 9). Answering to the questionnaire each expert voted for all of the statements grading every item on a 5 point scale according to Delphi method. 1=total disagreement, 2=disagreement, 3=agreement, 4=more than agreement, 5= total agreement. Consensus is reached when the sum of items “1”+“2” or “3”+“4”+“5” exceeds 66%. We called a Negative consensus if 1-2> 66%, positive consensus=3-4-5>66%, nonconsensus=1-2 or 3-4-5<66%.
As a result of the diccussions and the voting process the statements were modified and published as recommendations of the WFNS Spine Committee.
RESULTS
1. Rehabilitation for SCI
1) Physiotherapeutic treatment
Physical methods of treatment are aimed at restoring the function of the musculoskeletal system, preventing contractures, decubital trophic ulcers, accelerating regenerative and reparative processes, increasing the compensatory capabilities of the body, restoring the function of the pelvic organs. In the recovery and late periods, SCI is prescribed electrophoresis of antiinflammatory, mediator and vasodilator agents, ultrasound therapy, muscle electrical stimulation, magnetotherapy, hydromassage and mud therapy, hydrotherapy and balneotherapy.
(1) Massage: Short massage sessions (for example, 3 minutes) of the triceps muscle of the lower leg lead to a decrease in H-reflexes, but this effect lasts no more than a few minutes [1].
(2) Cryotherapy: Some studies report that cryotherapy can reduce muscle spasticity for up to one hour after stopping cold stimulation [3,4].
(3) Laser therapy: According to one randomized controlled trial, stimulation of sensitive nerve endings with a helium-neon laser for 40 seconds suppresses ankle clonus for up to 60 minutes [5].
(4) Exercise therapy [6]: One of the main tasks of medical rehabilitation of patients with patient-specific mobility therapy (PSMT) is the activation of movements and the partial or complete restoration of locomotion [7,8], therefore, along with other rehabilitation measures, the main role in the rehabilitation process is given to exercise therapy [6,9-14].
The use of motorized passive bicycle training normalizes the electrophysiological activity of motor neurons, reduces the level of spasticity [15].
Repeatedly walking exercises with the assistance of doctors or with the help of controlled orthoses while walking on a treadmill with unloading of body weight contribute to the restoration of walking after an incomplete injury to the spinal cord [9].
The many therapeutic simulators that have appeared in recent years have greatly expanded the possibilities of mechanotherapy and brought it to a qualitatively new level [16,17].
Walking on a treadmill with unloading body weight (bodyweight-supported treadmill training, BWSTT), according to many researchers, is one of the main methods of forming walking skills, training targeted, specific action [2]. Physiotherapy exercises or the BWSTT system helps to restore the ability to walk in more than 90% of patients with the level of lesion C [18,19].
(5) Hydrotherapy: Hydrotherapy is the external use of fresh water for therapeutic and prophylactic purposes in the form of various procedures, the most common of which are showers and baths.
Hydrokinesitherapy is an effective measure to improve mental functions and professional adaptation in people with psychiatric, behavioral and emotional disorders in PSMT. The main forms of hydrokinesitherapy: exercise therapy in water (therapeutic swimming, gymnastic exercises in water, training in walking, moving the body into an upright position and breathing exercises), underwater traction [20-22].
Contraindications to hydrokinesitherapy are open wounds, granulating surfaces, trophic ulcers, postoperative fistulas, acute and chronic skin diseases, eye diseases, ENT (ear, nose, and throat) organs, conditions after previous infectious diseases and chronic infectious diseases in the presence of bacillus carriage, sexually transmitted diseases, trichomonas colpitis, epilepsy, vertebrobasilar insufficiency with sudden loss of consciousness in history, exacerbation of chronic diseases, diseases of the upper respiratory tract, especially with hypersensitivity to chlorine, incontinence urine and feces, excessive sputum production, rheumatic heart disease in the acute stage, chronic nonspecific lung diseases in stage III, severe chronic coronary insufficiency, diseases of the cardiovascular system and other organs in the decompensation stage, acute inflammatory diseases of the kidneys and urinary tract, gallstone and urolithiasis.
(6) Balneotherapy (pool, bathtubs, showers): There is evidence of the second level that balneotherapy reduces spasticity and pain, improves cognitive functions, improves immunity, reduces fatigue, anxiety [23-29].
(7) Hyperbaric oxygenation [30,31]: Hyperbaric oxygenation is used to accelerate the recovery processes and therapy of concomitant pathology in patients with PSMT. Another method of medical rehabilitation is used. Oxygenobarotherapy eliminates the causes of ischemic disorders of the structures of the spinal cord and restores oxygen metabolism in ischemic brain tissue, which helps to improve motor activity of patients with SCI after a course of hyperbaric oxygenation.
2) Treatment of complications of SCI in the recovery and late periods
(1) Decubital trophic ulcers: Decubital trophic ulcers can occur in 43%–90% of adult patients with PSMT. The foci of decubital trophic ulcers significantly impede the implementation of rehabilitation measures, increase the material costs of care, treatment and rehabilitation of patients. The risk of developing decubital trophic ulcers is assessed according to the Waterlow scale.
For the treatment of decubital trophic ulcers, bioplastic material based on native type I collagen is used (the choice is “Kollost”) [32,33].
To judge the dynamics of wound healing, a photographic wound assessment tool [34] can be used in the wound assessment battery.
(2) Neurogenic bladder: There are different forms of urinary bladder according to violation of the function of the pelvic organs: (a) Normoreflex bladder: Urination occurs with a normal volume of the bladder in conditions of normal, decreased or increased tone. (b) Hyporeflex bladder: There is a low intravesical pressure, decreased detrusor strength and a sharply inhibited urination reflex, leading to overstretching of the bladder and a large amount of residual urine. (c) Hyperreflex bladder: Emptying the bladder is an automatism, accompanied by stressful or imperative urinary incontinence. (d) Areflex bladder: There is no cystic reflex, overstretching of the bladder or true urinary incontinence [35,36].
Therapy of neurogenic bladder must aim maintaining low pressure in the bladder, eliminating urinary incontinence, and reducing, if possible, the risk of impaired function of the upper urinary tract and their infection. Antibiotics are indicated only for symptomatic bacteriuria or exacerbation of a chronic infection a neurogenic bladder [35].
For a dynamic monitoring of the neurogenic bladder function in SCI the following measures must be applied: (a) Ultrasound of the kidneys annually to check for hydronephrosis; (b) Annual assessment of renal function: the main metabolic panel of biochemical blood tests (Chem 7: urea nitrogen, СО₂, creatinine, glucose, chlorides, potassium and sodium); (c) Cystoscopy with a permanent catheter every 10 years to exclude bladder cancer.
(3) Vegetative dysreflexia: Vegetative dysreflexia is a powerful sympathetic response that occurs in response to pain or other stimuli in patients with spinal cord damage above Th6. According to different authors, this syndrome is observed in 48%–83% of cases patients with tetraplegia and usually develops ≥2 months after injury [35].
Observation and treatment of vegetative dysreflexia can be done by following techniques. Arterial pressure and pulse are measured, patient’s head is raised to reduce intracranial pressure, squeezing clothing is loosened, a constant bladder catheter is placed.
(4) Heterotopic ossification: Heterotopic ossification is the process of the formation of benign bone tissue outside the skeleton. Ectopic ossificates usually form in the first 6 months after an injury in 10%–20% of patients and develop in areas located below the neurological level of the lesion. It is recommended to carry out computed tomography and scintigraphy. The treatment is complex and includes exercise therapy, therapeutic, radiation and surgical correction methods. The “gold standard” for pharmacological prevention of heterotopic ossification is indomethacin. The optimal time to start therapy is the first 2 months after the injury, the duration of treatment is 4–6 weeks. The standard dose of long-acting indomethacin is 75 mg daily, short-acting 25 mg 3 times a day. Numerous studies have shown the effectiveness of bisphosphonates for the primary prevention of heterotopic ossification in SCI. Etidronate is effective for primary prevention, as well as reducing heterotopic ossification both in the early and later stages of the disease. Radiation therapy and surgical excision of ossifications are the other optons. However, immature ossifications can recur, and resection of mature ossifications can lead to impaired joint function [35,37,38].
3) Provision of rehabilitation care for SCI
There are 3-stages for the provision of rehabilitation care for SCI:
Step 1. Rehabilitation measures in the acute period of injury: Transfer from the neuroresuscitation department to a multidisciplinary neurosurgery or traumatology hospital.
Step 2. Rehabilitation in the early and intermediate periods of injury: Specialized rehabilitation center for patients with dysfunctions of the central nervous system, peripheral nervous system and musculoskeletal system. It may last as long as indicated for up to 90 days.
Step 3. Rehabilitation in the late period: It includes dynamic observation with periodic medical rehabilitation courses. The clinic should better be at the place of residence of the patient. Mobile teams of rehabilitation centers for social protection can organize long-term medical and social patronage.
Routing patients with spinal injury through the stages of medical rehabilitation need a fine organization. Patients are referred for medical rehabilitation by specialists, as well as district physicians, general practitioners (family doctors). The doctor determines:
Medical indications and contraindications, stage and rehabilitation institutions (outpatient, inpatient, or spa);
Quantitative assessment of rehabilitation potential (RP) and assessment of RP in dynamics using a single equal-weighted scale in accordance with the International Classification of Functioning, Disability and Health [39].
In clinical practice, the following are also used to determine RP and functional capabilities of patients undergoing SCI: American Spinal Injury Association (ASIA) Scale, PULSES Profile test, Spinal Cord Injury Functional Ambulation Inventory, index Hauser’s walk, Standing balance test, Disability Assessment Scale, Functional Independence Measure, Barthel Index, modified Ashworth Scale, Tardieu Scale (Table 1) [36,38,40-42].

Scales used in the clinical practice to determine rehabilitation potential and functional capabilities of patients with SCI
Stages of developing an individual program of social rehabilitation of the patient should contain first an expert diagnosis of social status; RP assessment; definition of activities and services aimed at expanding the sphere of life; the implementation of social rehabilitation services in stages and continuously in a speciialized rehabilitation institution. The content and duration of the rehabilitation process are determined by the needs of the patient. One of the most important conditions for the effectiveness of the rehabilitation process is compliance with the rules of nursing care. Types of therapy in accordance with an individual rehabilitation program for a disabled patient are medication therapy, physiotherapy, mechanotherapy, kinesitherapy, hydrokinesisotherapy, psychotherapy, occupational therapy, walks, near and far tourism, exercise therapy and massage and manual therapy.
(1) Risk factors for rehabilitation
Rehabilitation departments must also fight against some medical problems that confront an active rehabilitation program. Some of these risk factors are acute and chronic somatic diseases in the stage of exacerbation or decompensation, infectious diseases, skin diseases, severe concomitant diseases that impede medical rehabilitation such as: cardiac diseases, uncontrolled arterial hypertension, respiratory problems, chronic renal failure, uncontrolled diabetes mellitus, malignant neoplasms.
Besides, mental illness, dementia, epilepsy, malnutrition, drug addiction and alcoholism, bleeding of various origins, pregnancy, unresolved spinal cord compression would prevent the use of rehabilitation necessary for patients with SCI.
To assess the nutritional status [43,44], anthropometric (body weight, height, body mass index [BMI], shoulder muscle circumference) are determined, laboratory (protein markers: total protein, albumin, prealbumin, transferrin, retin-binding protein), immunological (absolute number of blood lymphocytes) indicators, creatinine-growth index (based on daily excretion of creatinine with urine), urine urea nitrogen, and bioimpedansometry. The energy requirement of an organism is determined by indirect calorimetry using the consumption of О₂ (VO₂) and the release of CO₂ (VCO₂) using a metabolograph or calculated using the Harris – Benedict formula. A study at rest, with passive and active motor load, allows you to calculate not only exercise tolerance and energy capabilities of the body, but also the energy “cost” of individual motor acts.
Diagnosed outpatient nutritional deficiency is also based on the following clinical signs: a decrease in the patient’s body weight by more than 10% in 1 month. or 15% in 6 months, BMI < 18 kg/m², serum albumin < 30 g/L, patient’s inability to eat for more than a week, or a patient’s daily meal that provides less than 60% of the amount of energy he needs.
The choice of access for enteral nutrition is determined by the ability to independently receive the necessary nutrients through the mouth (sipping). If the latter is impossible, the type of enteral nutrition is determined by the degree of gastrointestinal damage (dysfunction) (nasogastric, gastrostomy, nasoduodenal, jejunostomy, nasojejunal accesses are carried out by installing special probes for enteral nutrition).
A significant contraindication to rehabilitation is the lack of motivation and urgent conditions. The degree of motivation to restore damaged functions is determined by the questionnaire “Restoring the locus of control” [45] - an instrument for indirectly assessing the level of patient motivation to recover. The test is based on the opinion of the patient regarding his role in recovery. Having read the options proposed in the questionnaire, the patient must express his agreement or disagreement with each of them.
Medicо-social rehabilitation of patients and disabled people with SCI should better be applied in the second and third stages. The development of an individual program of social rehabilitation of a patient includes the following stages: conducting rehabilitation and expert diagnostics of social status, evaluating RP, determining activities and services aimed at expanding the sphere of life. The specific types, volumes, forms and terms of the provision of services are determined taking into account the social status of the disabled person and the social rehabilitation program, which is part of an individual rehabilitation program. The effectiveness of medical and social rehabilitation services is characterized by the expansion of social functioning, the emergence of the ability to self-care, communication, the possibility of returning to professional activity.
Social rehabilitation includes: socio-environmental rehabilitation, socio-psychological rehabilitation, socio-pedagogical rehabilitation, socio-cultural rehabilitation, social adaptation, socio-recreational activities, and sports.
(2) Statements and their consensus results
Statement 1: Timely detection and correction of malnutrition improves the prognosis of patients after SCI. This statement reached a 100% positive consensus (total agreement 8%, more than agreement 75%, agreement 17%.)
Statement 2: For patients with urinary retention after SCI, intermittent catheterization is recommended. This statement reached a 100% positive consensus (total agreement 46%, more than agreement 36%, agreement 18%.)
Statement 3: Biodegradable collagen type I is effective in the treatment of decubital dystrophic ulcers. This statement reached a 100% positive consensus (total agreement 27%, more than agreement 27%, agreement 46%.)
Statement 4: Permanent and continuous physical therapy is recommended to patients in the second and third stages of medical rehabilitation. This statement reached a 100% positive consensus (total agreement 17%, more than agreement 42%, agreement 41%.)
Statement 5: Hydrotherapy, when feasible, is recommended for patients with SCI. This statement reached a 91% positive consensus. Positive consensus (total agreement 9%, more than agreement 18%, agreement 64%, disagreement 9%)
2. Functional Electrical Stimulation for SCI
Electrical stimulation methods are widely used in the restoration of motor functions after SCI [46,47].
SCI patients may benefit from functional electrical stimulation (FES). This form of physical therapy uses computer technology to send low-level electrical impulses to specific muscles in the patients’ legs, arms, hands or other areas. The electrical stimulation can cause muscles to contract, which may promote increased muscle bulk or muscle control. The muscle activity may also help reduce muscle spasms.
The nervous system is capable to change in response to electrical stimulation. Permanent changes are possible to be achieved with long-term and repetitive exposure. This phenomenon is known as neuronal plasticity. The amount and type of activity plays a critical role in both development and neuronal plasticity plasticity within the central nervous system. The dependence of development and plasticity in the Central Nervous System (CNS) on neural activity suggests that optimized neural activity might also be important for neural regeneration. There is evidence supporting this concept demonstrated by the fact that increased or decreased neural activity enhances or inhibits multiple components of spontaneous regeneration [48,49].
Clinically, a significant number of individuals with so-called complete SCI retain some connectivity across the injury site due to existence of myelin and/or denuded axons. Based on the above one can expect conductivity across the injury site, provided there is appropriate stimulation [50].
At present there is available research suggesting that patients who were regularly treated with FES demonstrated improved lower limb ASIA motor and sensory scores, also decreased spasticity [51,52].
There are 3 main types of electrical stimulation in use in the contemporary medical practice:
(a) Neuromuscular electrical stimulation is electricity applied across the surface of the skin over an intact peripheral nerve, which evokes action potentials.
(b) FES is the application of electrical stimulus to injured nerve attempting to restore or achieve function.
(c) Transcutaneous electrical nerve stimulation is used for pain modulation by exciting peripheral nerves using sensory, motor, or noxious settings, usually used to treat and alleviate back pain, neurogenic pain, arthritic pain, etc. pain.
In this paper the exposition will be focused mainly on the functional electric stimulation. There is wide variety of applications attempted for the FES, among which the following benefits can be achieved: maintain or increase the range of motion, reduction of swelling and edema, promotion of fracture healing or soft-tissue healing, reducing muscle spasm and the effects of spasticity, improving blood circulation, preventing or reversing the disuse atrophy, facilitate movements and neuromuscular reeducation.
The ideal patient for FES is considered to be a patient with upper motor neuron dysfunction in the settings of SCI. Results for the patients with lower motor neuron (LMN) dysfunction are dubious, but some clinicians still consider using it. The main stream of the clinicians consider that preservation of the entire LMN is essential for FES, thus LMN injury patients are not suitable for FES [53,54].
Contraindications for FES are considered as: Implanted electrical device, cancer, osteomyelitis, epilepsy, pregnancy. Different FES systems are currently developed for different problems.
1) FES for upper limb: surface and implantable devices
Many patients with C5 and C6 level tetraplegia have preserved LMN for C7 and C8 neurological segments and can benefit by both surface and implantable FES systems that is believed to have potential of restoring a degree of hand grasp, hold and release function, shoulder stability (for C4 level), elbow control [55].
2) FES for lower limb: surface and implantable devices
In 1963, Kantrowitz reported that person with paraplegia could stand during electrical stimulation of both quadriceps muscles simultaneously, however despite multiple attempts of various research groups, there is no FES system to allow complete SCI patient to walk to date. Achievements had been made in the support of standing and transfers but FES still can not replace the wheelchair [55-58].
3) FES systems for respiratory muscles: Patients with high cervical (C4) injury
Electrical stimulation of phrenic nerves functional stimulations of high cervical injury patients is applied in attempt to achieve or stabilize ventilator-free breathing, a technique generally referred to as electro-phrenic respiration or sometimes as phrenic nerve pacing [59].
4) FES systems for bladder, bowel and sexual function
FES is attempted also for contraction of the urinary bladder by electrical stimulation of the pelvic nerves. The technique was reported as early as the midnineteenth century. This observation led to attempts to improve micturition in patients with SCI by stimulation of the conus medullaris, sacral nerve roots, pelvic nerves or even the bladder itself, usually with dubious and unsatisfactory results.
The application of FES systems is known to have good impact on the general health of the patients with SCI as well. Among the most prominent general health benefits are the following:
(a) Cardiovascular conditioning: As per the available published literature, FES exercise has a potential to produce a twofold increase in the oxygen uptake, three-fold increase in ventilation rate, 5 beats per minute increase in heart rate from the resting value in volunteers with C5 to T12 SCI [60,61].
(b) Muscle and bone response: One of the most well-studied aspect of FES training may be the muscle and bone response. It is now well known that FES has a significant potential of muscles improvement in size, strength, and composition. Researchers found similar results with FES compared to training 2 to 3 times per week for 6 months at 30 or 50 rpm. Not the last FES achieves also beter cosmetic effect for the lower extremities in SCI patients [62-64].
(c) Recovery of lost bone mass: This is another very well-studied response. The recovery of lost bone mass is well demonstrated especially in the lower extremities, when the patients are subjected to FES treatment. Improvements in muscle mass and bone density may lead to fewer life-threatening conditions like fractures, pressure ulcers and infections [65,66].
(d) General health medical benefits: This is also reported as a result of FES. Among the reported metabolic benefits well known to be related to a good general health are decreases in adipose tissue, decrease of the blood glucose levels, decreased insulin levels, reversed course of the femoral artery size reduction and decreased wall compliance associated with SCI paralysis [65].
The published to date research suggest that FES applied to SCI patients may have a potential to improve the range of motion of the affected muscles and joints, prevent contractures, improve the muscular size and strength, improve the functional use of the hands, arms or legs. FES may also be associated with improved blood circulation and general heart health, improved aerobic conditioning and overall fitness level. A well-studied response to FES is ability to prevent loss of bone density which may lead to fewer life –threatening conditions like fractures, pressure ulcers and infections.
Unfortunately, all the published literature and conclusions are based on a small cohort studies and observational studies with no randomized control studies published to date.
All the available recommendations regarding the application of FES, found in the literature are with strength GRADE C or below.
5) Statements and their consensus results
Statement 6: FES is promising and in adjunct to rehabilitation may improve:
- Range of motion, muscle size and strength
- Functional use of the hands, arms or legs
- Blood circulation and health of the heart
- Aerobic and metabolic conditioning and overall fitness levels
- Ability to prevent loss of bone density and thus preventing life-threatening complications (fractures, pressure ulcers, infections)
This statement reached a 100% positive consensus (total agreement 23%, more than agreement 54%, agreement 23%.)
3. Spasticity and Pain Management After SCI
Current statistics show that around 65% to 85% of all patients with SCI might present pain and one third of these may progress to chronic and severe pain that is difficult to manage, and that could be refractory to medical management and required surgical procedures. The most frequent form is central or neuropathic pain that is characterized by burning tingling pain below the level of the spinal injury (Table 2) [67,68].

Classification of pain related to SCI
1) Spinal cord stimulation in patients with pain associated with SCI
Spinal cord stimulation can improve neuropathic pain and musculoskeletal pain associated with SCI. Cioni et al. [69] reported the implantation of epidural electrodes on the posterior cords of the medulla for stimulation.
There is grade 4 evidence from a case-control study that spinal cord stimulation improves neuropathic pain in patients with squealae of SCI [68].
The main indications in spinal cord stimulation are in patients with failed spine surgery syndrome and complex regional painful syndrome. There is no better evidence to grade 4 that supports the use of spinal stimulation in patients with other types of pain [70,71].
It is very important to select a patient who can benefit from spinal stimulation surgery: active medullary dorsal cords, measured by normal central conduction times, a complete psychological evaluation is required, and to rule out comorbidities including opioid dependence and the risk of infections [71].
2) Dorsal longitudinal t-myelotomy for pain management after SCI
Livshits et al. [72] report in a case-control study comparing the Pourpre versus Bischof II approaches and assesses the effectiveness of reducing pain and refractory spasticity in patients with SCI (N = 40), the follow-up at 6 months, 5 and 10 years using the McGill Pain Questionnaire, the current intensity scale of the pain and the visual analogue scale (VAS) to assess control and improvement of pain, found that both techniques are effective for this purpose, however, with more significant results with the Pourpre technique [72].
There is level 3 evidence from a case-control study to support the use of longitudinal myelotomy to decrease spasticity with pain in patients with SCI [72,73].
The main indications for myelotomy are in patients with abdominal or pelvic visceral pain secondary to cancer.
3) DREZotomy for pain management after SCI
Dorsal Root Entry Zone Lesion, DREZotomy (DZT), was designed by Sindou et al. [74] in 1974 for the treatment of neuropathic pain of different origins, including: posttraumatic brachial plexus avulsion and segmental rachimedullary pain. The surgery consists of: destruction of A delta and C fibers, destruction of the excitatory medial part of the tract of Lissauer and destruction of the dorsal excitatory interneurons (First five Rexed’s layers) (Fig. 1). He also demonstrated its utility for the treatment of spasticity, deepening the lesion 1 mm to cut the fibers responsible for the myotatic reflex.
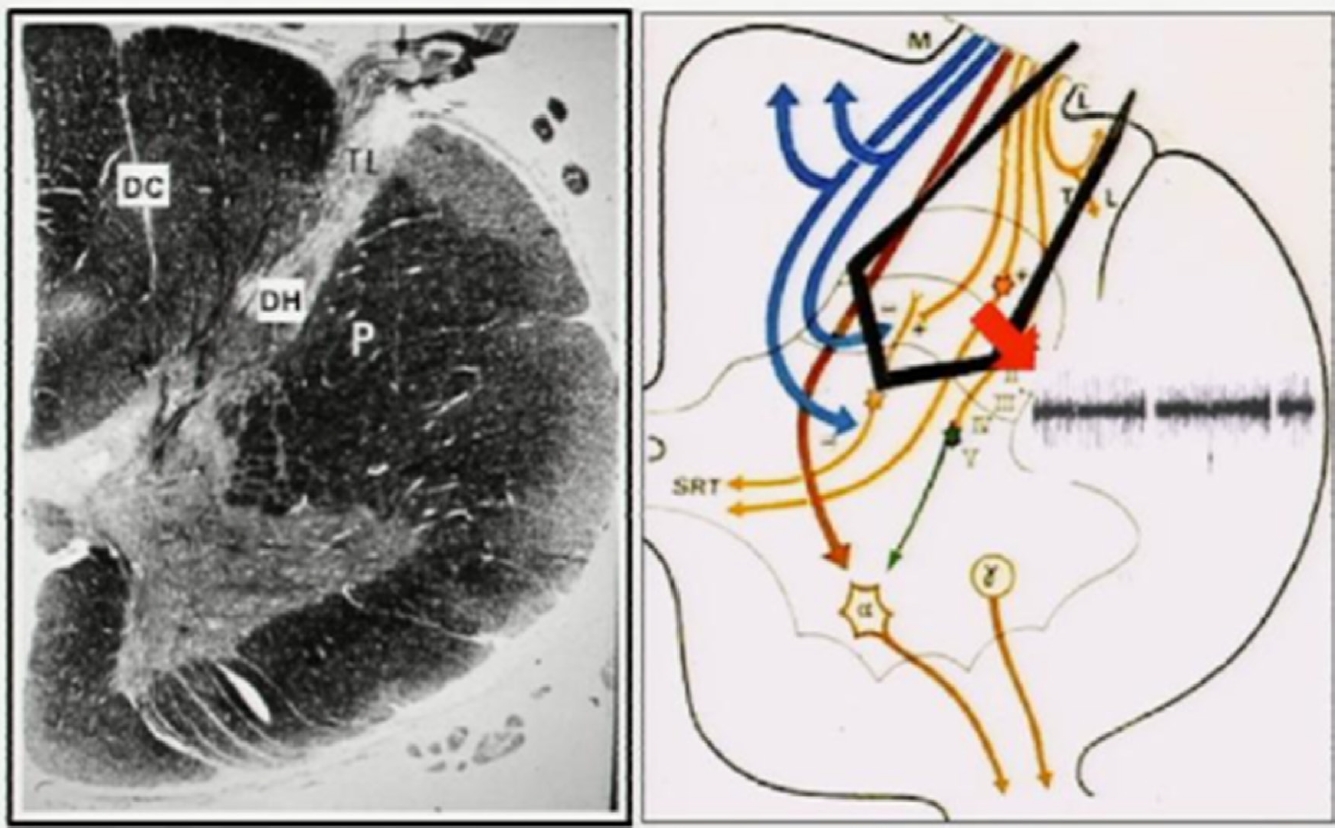
Organization of fibers on transverse section. Most of the fine (nociceptive) afferents, which convey excitatory input, enter the dorsolateral sulcus as a lateral bundle of the DREZ, then penetrate the dorsal horn (DH) ventrolaterally through the medial part of the tract of Lissauer (TL) and the dorsal aspect of the substantia gelatinosa (SG). The Ramón y Cajal’s recurrent collaterals of the large primary afferent fibers approach the DH through the ventromedial aspect of the SG to exert inhibitory effects on the DH neurons [75]. Because a number of dendrites of the cells of origin of the spinoreticulothalamic tract, which will form the contralateral anterolateral pathways, make synaptic connections with the primary afferents inside the SG layers, the SG exerts a strong segmental modulating effect on the nociceptive input.80 Arrowhead: The microsurgical DREZotomy (MDT) target includes the lateral bundle of the (nociceptive) fine fibers, the medial (excitatory) part of the TL, and the 5 dorsalmost layers of the DH where the primary afferents terminate and whose neurons become hyperactive if deafferentated. MDT attempts to spare the máximum number of the large fibers of the medial bundle that reach the DC. Reprinted from Sindou et al. Pain 2001:92:159-71, with permission of Wolters Kluwer Health, Inc [75].
Sindou et al. [75] observed that in patients with chronic pain post SCI, the DZT only is effective in patients with pain of segmental distribution, with 68% cured, and DZT is not effective for pain in the territory below the lesion, especially when located in the perineo-sacral area, even if DZT is performed below the lesion in the lower medullary segments (Fig. 2).
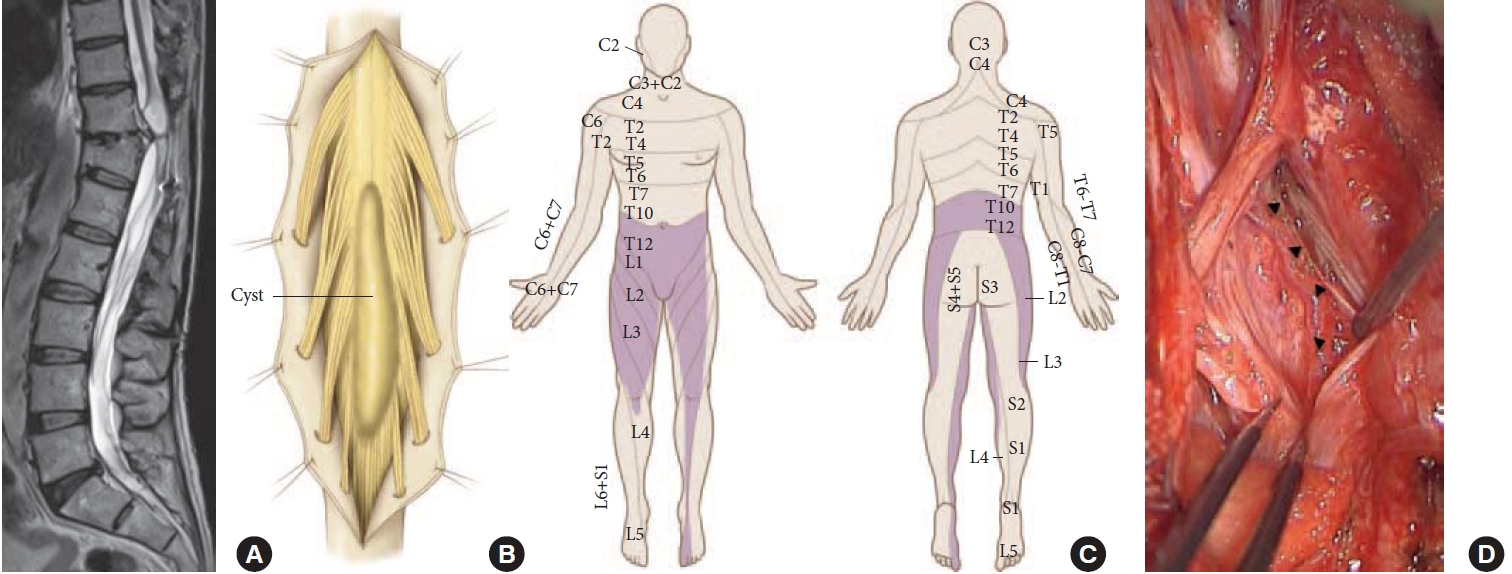
Microsurgical DREZotomy (MDT) for spinal cord and cauda equina injury. MDT is performed bilaterally in a paraplegic patient after spinal cord injury at the conus medullaris (A), with a crush of T12 to L4 spinal segments presenting with “segmental pain” in the corresponding territory (C). The drawing (B) illustrates the intraoperative findings: myelomalacic cyst and gliosis in the conus medullaris. MDT will be performed at the T12 to L4 spinal cord segments, bilaterally. The operative view (D) shows fibrotic arachnoids surrounding the conus medullaris and cauda equina roots as well as the contused spinal cord. Arrowheads designate the dorsolateral sulcus, which was difficult to identify within the fibrotic arachnoid and gliotic cord. Reprinted from Sindou et al. Pain 2001:92:159-71, with permission of Wolters Kluwer Health, Inc [75].
Other authors working on the same problem, Nashold and Ostdahl 76 demonstrated the difference of the technique of DREZ coagulation from DREZotomy that Dr. Sindou first desinged (Fig. 3). He worked with patients with avulsion of the cervical dorsal roots of the brachial plexus and intractable pain.

The DZT main indications are patients with avulsion injury of the brachial plexus and segmental pain in patients with SCI [73,74,75].
There were 11 studies found that evaluated the effectiveness of DREZotomy to reduce neuropathic pain in patients with SCI [70]. In general, all demonstrated that it can be effective for this purpose, however, because the level of evidence is not strong enough, these results should be carefully evaluated. The majority of the studies did not have a cohort group and were mainly observational; the inclusion of a cohort group in this type of procedure may have ethical questions.
Falci et al. [77] conducted a study with 2 groups; 9 patients were treated with microcoagulation drezotomy using spinal neuroelectrical hyperactivity, while the other group underwent the same procedure but using registered and evoked spontaneous hyperactivity as a guide. Patients were evaluated at 6 years using the VAS in a cohort-study. In the second group 80% presented improvement of pain compared to a 50% in patients of the first group [70].
Lee et al. [78] reported 38 patients with different types of neuropathic pain, both segmental and diffuse pain treated with drezotomy with an average follow-up of 42 months. Using the VAS, it was found that patients with intermittent pain and patients with continuous pain presented high rates of pain improvement 78% and 80%, respectively [68].
There is level 2 evidence to support the use of DZT in the management of patients with pain associated with SCI. The results are better in patients with segmental pain vs. diffuse pain [70,73,74,75]. Also when the segmental pain is associated with spasticity [73,75].
4) Intrathecal baclofen for the management of spasticity in patients with sequelae of SCI
Mcintyre in their systematic review showed that there are several studies that report improvement of spasticity by SCI with the use of intrathecal baclofen. However, all are evidence level 4 [79].
Currently, there are several procedures described in the surgical management of neuropathic pain associated with spinal cord trauma. The best evidence is the DREZotomy procedure for the treatment of segmental pain and spasticity associated to SCI, which has grade 2 evidence studies. The other procedures described in the literature do not have strong evidence to support their use in all patients.
5) Statements and their consensus results
Statement 7: DREZotomy should be the prefered treatment option for the management of refractory pain and spasticity in patients with complete SCI. This statement reached a 86% positive consensus (total agreement 14%, more than agreement 29%, agreement 43%, disagreement 14%).
Statement 8: For patients with total SCI, dorsal myelotomy is a therapeutical option. This statement reached a 93% positive consensus (total agreement 14%, more than agreement 43%, agreement 36%, disagreement 7%).
Statement 9: Spinal cord stimulation may be an option to treat chronic neurophatic pain secondary to SCI. This statement reached a 93% positive consensus (total agreement 8%, more than agreement 8%, agreement 77%, disagreement 7%).
Statement 10: Intrathecal Baclofen may be an option for the treatment of spasticity secondary to SCI. This statement reached a 91% positive consensus (total agreement 18%, more than agreement 55%, agreement 18%, disagreement 9%).
CONCLUSION
SCI is a complex condition associated with significant disability, causing reduction in the quality of life, and significant expences to adjust and maintain the normal functioning. The care for the SCI has gone a long way from the times after the World War II when these patients were considered hopeless in terms of any functional recovery, to the contemporary comprehensive rehabilitation programs, achieving significant success in resocialising. Complications of the SCI such as pain and spasticity can be diminished by some surgical techniques we discussed. The current manuscript reflects different aspects of the contemporary rehabilitaton process and decision makings, which were discussed by the faculty of the WFNS Spine Committee resulting in issuing of the following recommendations. Each of the recommendations were scrutinized and voted upon by the committee.
WFNS SPINE COMMITTEE RECOMMENDATIONS
Recommendations for Rehabilitation for SCI
• Timely detection and correction of malnutrition improves the prognosis of patients after SCI.
• For patients with urinary retention after SCI, intermittent catheterization is recommended.
• Biodegradable collagen type I is effective in the treatment of decubital dystrophic ulcers.
• Permanent and continuous physical therapy is recommended to patients in the second and third stages of medical rehabilitation.
• Hydrotherapy, when feasible, is recommended for patients with SCI.
Recommendations for FES
• FES is promising and an adjunct to rehabilitation. It may improve:
The range of motion, muscle size and strength
Functional use of the hands, arms or legs
Blood circulation and health of the heart
Aerobic and metabolic conditioning and overall fitness levels
Ability to prevent loss of bone density and thus preventing life-threatening complications (fractures, pressure ulcers, infections)
Recommendations for Spasticity and Pain Management After SCI
• DREZotomy can be a good treatment option for the management of central pain and spasticity in patients with complete SCI.
• Dorsal myelotomy is a therapeutical option for patients with complete SCI having spasticity and pain.
• Spinal cord stimulation may be an option to treat chronic neurophatic pain secondary to SCI.
• Intrathecal Baclofen may be an option for the treatment of spasticity secondary to SCI.
Notes
The authors have nothing to disclose.