INTRODUCTION
As the elderly population continues to grow, an increasing number of people suffer from lumbar degenerative disease (LDD), which causes pain and disability. Spinal fusion is considered an effective technique for treating LDD, and this technique is continuously developing to achieve the goal of maximizing outcomes and minimizing morbidity. Minimally invasive spinal (MIS) surgery has gained popularity among spinal surgeons because of advances that reduce intraoperative trauma, require smaller incisions, require less recovery time, and result in fewer perioperative complications [1,2]. Spinal endoscopy techniques have developed rapidly and are widely used in treating LDD. A newly emerging endoscopic spinal surgery, endoscopic transforaminal lumbar interbody fusion (Endo-TLIF), is manipulated via the transforaminal corridor with little bone removal and maximum preservation of the surrounding structures [3,4]. Many previous studies have suggested that Endo-TLIF is an effective and safe procedure for LDD [5-7].
However, as in other MIS surgeries, fluoroscopic assistance is essential for Endo-TLIF because surgeons must reach the proper target and place the pedicle screws percutaneously. In fact, fluoroscopy is used both in the first step and throughout the procedure because it is difficult to identify the operation direction through the percutaneous pathway. In addition, further fluoroscopic checks are required for the insertion of the polyetheretherketone (PEEK) cage and fixation of the pedicle screws. Therefore, intraoperative radiation exposure for both patients and surgeons is of significant concern.
In recent years, navigation systems have been successfully applied in various surgical fields [8] including neurosurgery, endoscopy, bronchoscopy, and arthroscopy. They are also used in spinal surgery, and many studies have suggested that they can effectively reduce radiation exposure and surgical time [9-11].
There have been very few studies on the navigation systems used in Endo-TLIF. Therefore, we aimed to introduce Endo-TLIF using the O-arm-based navigation system and compare the results between the navigation and fluoroscopy groups.
MATERIALS AND METHODS
We retrospectively analyzed 64 patients who underwent Endo-TLIF assisted by O-arm navigation or conventional 2-dimensional (2D) fluoroscopy in our center between May 2019 and September 2020. The Ethics Committee of the Second Affiliated Hospital of Army Medical University approved this study, and written informed consents were obtained from all patients. Patients who met all of the following criteria were included: (1) age Ōēź 18 and Ōēż 80 years, (2) diagnosis of lumbar spondylolisthesis (below Meyerding grade II), lumbar instability, or lumbar spinal nerve canal stenosis, and (3) conservative therapy for Ōēź 3 months prior. The exclusion criteria included inoperable physical ailments or mental disease, history of lumbar spinal surgery, spinal infection or tumor, and traumatic lesions. One experienced surgeon performed all the surgeries.
Perioperative data such as radiation dose, blood loss, postoperative drains, surgery time, complications, and length of hospital stay (LOS) were collected. In addition, the time required for specified steps in the surgery was recorded, including the navigation set-up time, cannula placement time, and percutaneous pedicle screw fixation time. Clinical outcomes were evaluated from postoperative data such as Oswestry Disability Index (ODI), visual analogue scale (VAS), and modified MacNab criteria. Surgical complications were assessed, including severe nerve root injury, vascular damage, hematoma, and cauda equina injury. Additionally, patient spine fusion was assessed using computed tomography (CT) images at 12 months postoperatively. The bridging trabecular bone formation between the vertebral body was regarded as solid fusion in the CT images. Radiation dose and surgery time were selected as primary outcomes, and the others were secondary outcomes. The radiation dose was collected from the radiation generator, and the duration of radiation exposure was also collected.
1. Endo-TLIF Assisted by O-arm Navigation Surgical Procedure
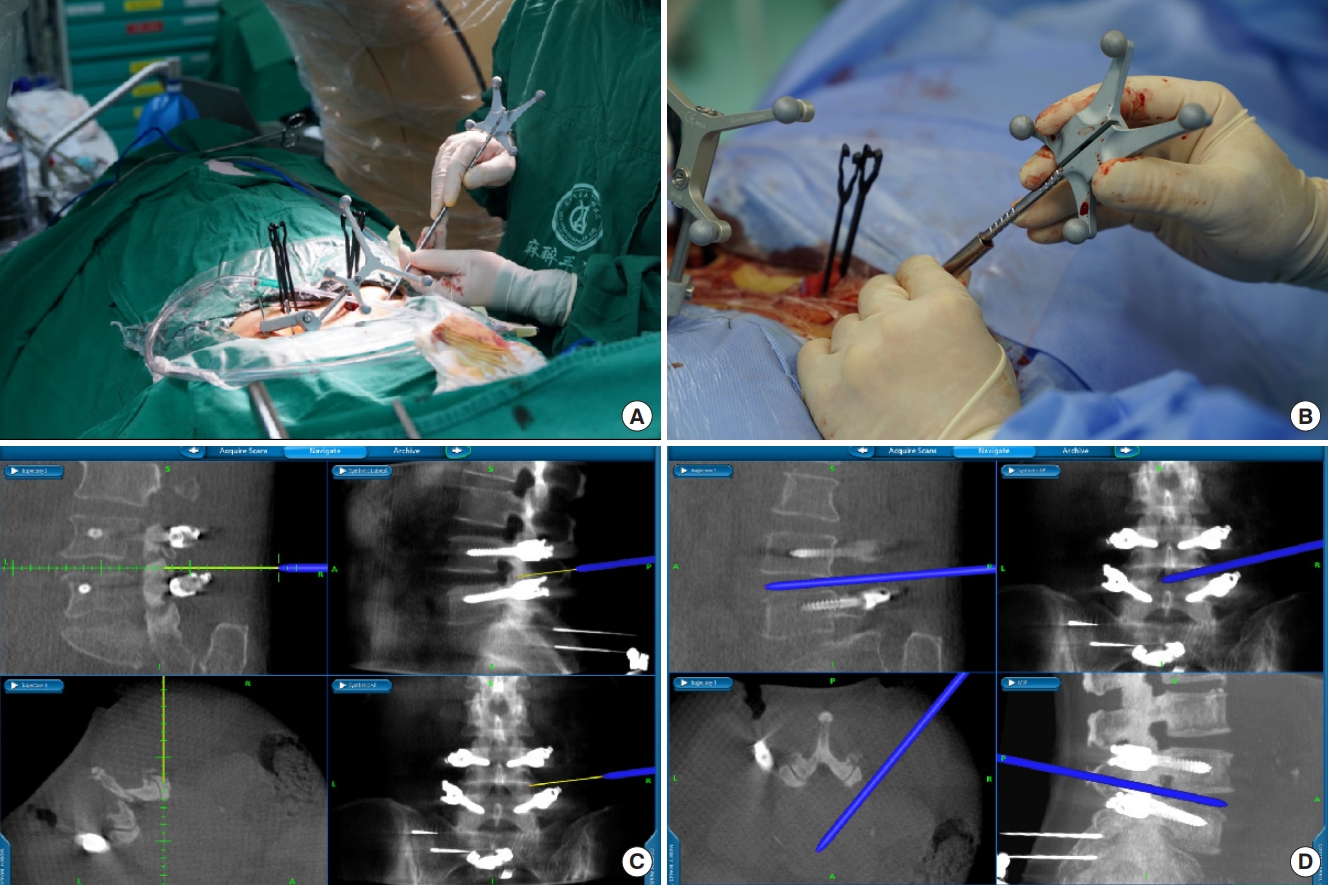
Patients with general anesthesia were placed in the prone position. A nerve monitoring system monitored somatosensory-evoked potentials and free-running electromyography throughout the operation. Two K-wires (2.0-mm diameter) were used to anchor the reference frame to the iliac crest (Fig. 1A). Next, the O-arm (O-arm Surgical Imaging System and Stealth-Station; Medtronic, Minneapolis, MN, USA) was used to obtain intraoperative 3-dimensional (3D) images (Fig. 1B). Then acquired CT pictures were instantly transmitted to the computer, and multiplanar images of the lumbar spine were reconstructed using the navigation system. Subsequently, surgical instruments were registered to be traced intraoperatively in real time. In general, navigation preparation time, including reference frame fixation, O-arm scan, picture transmit, and instrument registration, is less than 10 minutes.
The entry point of pedicle screws was determined using 3D-image guidance to optimize screw length and avoid neurovascular structures. The pedicle screw was placed at a suitable depth using a navigated screwdriver (Fig. 2A, B). The image of screw trajectory and position was displayed on the monitor in real time, and the surgeon could make appropriate adjustments according to the image (Fig. 2C, D). After the screws were in place, C-arm was used to confirm the final position of the screws. Next, we use a spinal needle to reach the target point via the navigation system. Sequential dilation was performed to expand the soft tissue, and a double-cannula device was docked on the lateral aspect of the facet joint to perform foraminoplasty under navigation guidance. The navigation system showed the depth and pathway of the reamer or bone drill on a computer screen in real time until foraminoplasty was completed (Fig. 3). After the working cannula was advanced through the dilator and its position was confirmed using C-arm, reamers of different diameters were used to remove the degenerative disc tissue. Thereafter, the intervertebral disc was filled with allografts and recombinant human bone morphogenetic protein, and PEEK cages were implanted via an expandable tube (ZELIF, Sanyou, China). The final position of PEEK cages was identified using C-arm. Finally, a standard percutaneous endoscopic lumbar discectomy procedure was performed.
2. Surgical Technique of Endo-TLIF Assisted by C-arm
The operation was performed with the assistance of traditional fluoroscopy, as previously reported [12]. After surgery, analgesic and anti-inflammatory treatments were administered.
3. Statistical Analysis
The IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA) was used to analyze data, and Statistical significance was defined as p-values less than 0.05. Statistics are expressed as mean ┬▒ standard deviation or frequency. The Independent-sample t-test, chi-square test, and Mann-Whitney U-test were used to examine differences between the 2 groups, as appropriate.
RESULTS
Thirty-four patients were included in the nonnavigation group (14 men and 20 women), and 30 patients in the navigation group (13 men and 17 women). The follow-up time of all patients was at least a year. No significant differences in patient demographics were detected between the 2 groups (Table 1).
The dose of radiation administered was 7.58 ┬▒ 0.84 mGy in the navigation group; this was significantly lower than in the nonnavigation group (59.08 ┬▒ 9.77 mGy). The duration of radiation exposure was 59 seconds in the nonnavigation group and 9 seconds in the navigation group (p < 0.001). Intraoperative blood loss, postoperative drainage, hospital LOS, and complications were not significantly different between the 2 groups (Table 1). The navigation set-up time was 5.9 ┬▒ 0.84 minutes. Both cannula placement time (22.6 ┬▒ 2.7 minutes) and pedicle screw fixation time (37.0 ┬▒ 2.8 minutes) were significantly shorter in the navigation group. The total operation time was also reduced in the navigation group (p < 0.001) (Table 2). Compared with preoperative scores, both VAS and ODI scores significantly improved after surgery at different times in both groups (Table 3). Nevertheless, there were no significant differences between the 2 groups (Table 3). The excellent and good rates were 91.2% in the nonnavigation group and 93.3% in the navigation group. No significant difference was observed between the excellent and good rates of the 2 groups (p = 0.682). No major complications occurred during the surgery. Only 2 occurrences of transient ipsilateral dysesthesia were recorded, and the clinical symptoms disappeared with conservative treatment. The spine fusion was 94.1% (32 cases) and 93.3% (28 cases) respectively in the nonnavigation group and navigation group at 12 months postoperatively, and no significant difference was observed between the groups. However, all patients in the 2 groups had achieved solid spine fusion at the final follow-up, and there was no subsidence occurrence in both groups.
DISCUSSION
As a minimally invasive procedure, Endo-TLIF has been successfully manipulated to treat LDD and achieve positive clinical outcomes [7,13]. Jin et al. [13] presented a consecutive case series of Endo-TLIF, demonstrating satisfactory clinical and radiological results. It indicated that Endo-TLIF is a promising surgical alternative for treating LDD. In 2020, Wu et al. [14] compared Endo-TLIF with open-TLIF in the treatment of LDD, supporting the hypothesis that Endo-TLIF is a viable option for treating single-segment LDD with little trauma, rapid recovery, and inexpensive cost. These both suggest that Endo-TLIF is an effective technique with less trauma and faster recovery. Intraoperative ionization-based imaging techniques are essential for MIS surgery to expose the spine visually. Compared with open procedures, x-rays are more frequently used during the operation, which increases surgery time and causes harm to both patients and medical staff [15,16]. Therefore, the associated radiation exposure remains a major concern, especially for surgeons who are frequently exposed [17].
Compared with open surgery, MIS techniques such as MIS-TLIF are highly dependent on fluoroscopy as the limited exposure fields and constrained working tube, which results in higher radiation exposure to both patients and the surgeon [18]. In a meta-analysis, the results indicated that mean fluoroscopy in MIS-TLIF was 94 seconds which was 2-fold of open surgery [19]. In addition, Godzik et al. [20] also reported that radiation exposure to the surgeon in the MIS-TLIF group was 408.3 ┬▒ 192.3 ╬╝Sv which was significantly higher than lateral transpsoas lumbar interbody fusion (208.6 ┬▒ 146.9 ╬╝Sv). A previous prospective cohort study [21] showed that Endo-TLIF had less intraoperative blood loss, less patient postoperative pain, and shorter hospital stay with similar surgical outcomes when compared with MIS-TLIF. These outcomes prove that Endo-TLIF is better than MIS-TLIF in certain diseases. However, as a less invasive surgery than MIS-TLIF, there are many other percutaneous procedures in Endo-TLIF besides percutaneous screw placement, leading to more radiation exposure. The advent and development of navigation technology have had a profound impact on spinal surgery [22,23]. Computer-assisted 3D navigation can provide high-resolution images and a more detailed view of the pedicles, improving the precision of spinal screw placement. As reported in a previous study, the nerve injury risk and clinical complications could be decreased through this technique [24]. Zhao et al. [25] compared the occurrence of postoperative hydrothorax between O-arm navigation and free-hand in spinal deformity surgery. They found that the volume of postoperative hydrothorax could be significantly reduced using the O-arm navigation, and this was ascribed to the improvement in screw implantation accuracy. Besides this, the O-arm navigation system can significantly reduce the radiation exposure of surgeons. Images can be obtained using navigation systems, with the surgeons outside the operating theater, with no additional intraoperative CT scan or fluoroscopy required to continue with the procedures. A prospective randomized study compared radiation exposure between 2D and 3D fluoroscopic techniques. The results suggested that the surgeon radiation exposure in the 2D fluoroscopy group was 9.96 times higher than that in the navigation group [26]. In the present study, the mean radiation dose in the navigation group was 7.58 ┬▒ 0.84 mGy, much lower than that in the nonnavigation group. Our results are consistent with those of a previous study [27].
In our study, although there is an additional mean 5.9-minute navigation set-up time before surgery, the total duration of surgery in the navigation group was significantly shorter than that in the nonnavigation group (119.8 ┬▒ 10.5 minutes vs. 134.2 ┬▒ 10.2 minutes). This may be ascribed to the reduced time of cannula placement (22.6 ┬▒ 2.7 minutes vs. 34.6 ┬▒ 3.7 minutes) and pedicle screw placement (37.0 ┬▒ 2.8 minutes vs. 47.1 ┬▒ 2.8 minutes) in the navigation group. The results showed that the efficiency of Endo-TLIF was improved by navigation. In another retrospective study, the effect of navigation on surgical efficiency was explored [28]. The total operative time decreased significantly in the O-arm navigation group compared with the free-hand group. In the present study, clinical outcomes such as VAS and ODI scores improved significantly in the 2 groups postoperatively. Differences between the nonnavigation and navigation groups were not detected significantly in the VAS and ODI scores. Also, hospital LOS and complications were not significantly different in the 2 groups. Several previous studies have assessed the impact of O-arm navigation on clinical outcomes (nerve injury and reoperation rate). These studies support the hypothesis that navigation-assisted spinal surgery could improve clinical outcomes by reducing nerve injury and reoperation rates for mispositioned screws [29-31]. All surgeries in our study were performed by senior doctors; hence, it was not difficult for them to place screws accurately in the lumbar pedicle. Therefore, we did not study the screw placement. No patients underwent reoperation in either of the 2 groups; only 2 occurrences of transient ipsilateral dysesthesia were recorded in the nonnavigation group, and the clinical symptoms disappeared with conservative treatment.
Endo-TLIF surgery assisted by O-arm navigation offers several advantages. First, the surgical efficiency could be improved, especially in some percutaneous procedures, including cannula placement and pedicle screw fixation. Second, the radiation exposure to operation staff can be reduced, having a positive effect on protecting their health. In addition, surgeons can determine the desired screw sizes and rod lengths and assess the extent of the discectomy. However, some disadvantages have also been reported. First, O-arm for intraoperative CT navigation resulted in higher radiation doses to patients compared with C-arm [32-34]. In a multicenter study, the results indicated that the mean doses for patients in the O-arm group were 4 times higher than those in the C-arm group [35]. Radiation exposure shows a positive dose effect in breast cancer mortality [36] and has been linked to various cancers [37]. Although some minimized-dose O-arm Protocols could be used to reduce negative effects for patients [38], the impact of exposure for patients in O-arm navigation remains a problem. Moreover, O-arm-assisted Endo-TLIF surgery is comparatively expensive and may lead to an additional financial burden on patients. Although the cost of new technologies is reducing steadily over time, more research on cost-effectiveness is needed to justify the navigation technique financially [39]. There are some limitations to our study. This was a retrospective study that compared the intraoperative data and clinical outcomes between the 2 groups. The sample size was relatively small, and inherent selected bias could not be ignored. Randomized controlled trials with large sample sizes and long-term follow-up are needed in future.
CONCLUSION
We have shown that Endo-TLIF assisted by O-arm navigation is efficient and can reduce radiation exposure. O-arm navigation could reduce radiation exposure and surgical time in Endo-TLIF surgery with clinical outcomes similar to those with fluoroscopy. Navigation is a promising alternative for patients undergoing Endo-TLIF surgery. However, the higher doses exposed to patients remain a negative effect of this technology.