Facet Articular Irregularity Is the Most Relevant Risk Factor for Rapidly Progressive Degenerative Cervical Myelopathy
Article information

Abstract
Objective
Facet articular irregularity is associated with rapidly progressive degenerative cervical myelopathy (DCM). However, its significance compared with other known risk factors remains unknown. Therefore, this retrospective study aimed to clarify the potential impact of facet articular irregularity as a risk factor for rapid DCM progression.
Methods
This study included 141 consecutive patients with DCM who underwent surgical treatment at our institution. Clinical variables and radiological findings related to DCM progression were collected. Imaging findings were analyzed at the segmental level of myelopathy in each case. The patients were divided into 2 groups based on the presence or absence of rapid DCM progression, and independent risk factors were determined using logistic regression analyses.
Results
Overall, 131 patients with a mean age of 63.9±12.6 years were analyzed; 27 patients (20.6%) were classified into the rapid DCM progression group. The mean age was significantly higher in the rapid progression group than in the slow progression group (72.4±9.6 vs. 61.7±12.4, p<0.001). According to univariate analysis, facet articular irregularity, dynamic segmental translation (≥1.6 mm), upper cervical spine involvement above C4–5, history of cerebrovascular events, preceding minor trauma, local lordotic angle (≥4.5°), diabetes, hypertension, ligamentum flavum hypertrophy, and age were independent risk factors. Additionally, multivariate analysis showed that facet articular irregularity was the highest risk factor for rapid DCM progression (p=0.001).
Conclusion
Facet articular irregularity is the most clinically significant finding among the known risk factors in patients with rapid DCM progression.
INTRODUCTION
Degenerative cervical myelopathy (DCM) is a common spinal disorder caused by osteoarthritic changes to the spine, including spondylosis, disc herniation, and facet arthropathy, ligamentous hypertrophy, calcification, or ossification [1]. Degeneration of the cervical spine is initially asymptomatic; however, it may gradually present with and may cause not only arthropathy but also myelopathy or radiculopathy. DCM, which is represented by cervical spondylotic myelopathy (CSM), is an age-related disease that reduces quality of life due to impairment of motor functions [2]. Additionally, DCM is a slowly progressive disorder that corresponds to the underlying degenerative changes [3-7]. However, it is known that some patients experience rapidly progressive neurological deterioration despite the absence of trauma [8,9].
The preoperative severity of myelopathy correlates with poor postoperative outcomes in patients with DCM, similar to those with CSM [10]. Therefore, in patients with rapid DCM progression, surgical intervention as early as possible is strongly recommended to prevent poor postoperative outcomes. To avoid neurological deterioration in such patients, it is important to identify risk factors that may predict rapid disease progression. However, few reports have described rapid neurological progression in DCM [8,9].
We recently reported, for the first time, that the degenerative pathology of the facet joint is potentially important, and that facet articular irregularity is a specific finding in cases of rapidly progressive DCM [11,12]. However, the impact of facet joint pathology in DCM is still controversial [13,14]. Thus, the importance of specific findings regarding facet degeneration remain unclear when compared to known factors involved in the progression of myelopathy. Therefore, this study was conducted to determine the predictive factors of rapid DCM progression and their order of relevance with factors involved in myelopathy progression, including facet articular irregularity: a newly known risk factor.
MATERIALS AND METHODS
All experiments were conducted in accordance with the Declaration of Helsinki. All research protocols were approved by the Institutional Review Board of Nara Medical University (approval number: 2241). The requirement for informed consent was waived since it was a retrospective study.
1. Patient Selection
We retrospectively analyzed consecutive patients with DCM who underwent surgical treatment at Nara Medical University between January 2013 and December 2020. The study population was the same as in the previous study [12]. Inclusion criteria included cervical myelopathy responsible for the subaxial level between C2–3 and C6–7. The diagnosis of cervical myelopathy was based on symptoms and magnetic resonance imaging (MRI) findings. The responsible segmental level was defined as the level of the lesion causing myelopathy and was identified in each case based on neurologic examinations and MRI findings, if necessary. Patients who had undergone revision surgery within 12 months or those with missing data were excluded.
Clinical data and radiological findings were gathered retrospectively from medical records, preoperative and postoperative neurological examinations, and radiographic images.
2. Clinical Data Collection
Clinical variables, such as age, sex, comorbidities (hypertension, diabetes mellitus, cigarette smoking, habitual alcohol use), background disorders, responsible spinal segmental level, pre- and postoperative Japanese Orthopaedic Association (JOA) scores for the evaluation of cervical compression myelopathy [15], and preoperative Nurick grade were collected from the patients’ records. Recovery rate (%) of the JOA score was also calculated using the following formula: (“postoperative score”-“preoperative score”)/(17-“preoperative score”)×100. Other clinical variables that are potentially involved in the rapid progression of cervical myopathy in DCM, such as history of cerebrovascular events (CVEs) and preceding minor trauma, were also gathered.
We also assessed the characteristic clinical course and rapid progression of cervical myelopathy in each case. Rapid progression of cervical myelopathy was defined in this study as previously reported [8,9,12]. In brief, patients with rapid DCM progression had difficulty maintaining a standing posture or walking without support, which corresponded to Nurick grade 4 or 5, within 4 weeks of symptom onset, due to rapidly progressive neurological deterioration.
3. Radiological Evaluations
Radiological variables potentially involved in the progression of cervical myopathy in DCM were gathered from preoperative computed tomography (CT) and MRI and radiograms of the cervical spine in each patient. From the MRI review, intramedullary hyperintense changes on sagittal T2-weighted images at the responsible segmental level (Fig. 1A), hypertrophy of the ligamentum flavum at the responsible segmental level (Fig. 1B), and the number of levels with spinal canal stenosis in each patient were assessed. From the CT review, we carefully evaluated the cervical disc and facet joints at the responsible segmental level and assessed the presence of calcified discs (Fig. 1C) and facet articular irregularity (Fig. 1D), which was defined as equivalent to grade 4 or 5B in the CT classification reported previously [12] at either or both facet joints.

Radiological assessments in the cervical spine on magnetic resonance image (A, B) and computed tomography image (C, D) at the responsible segmental level. (A) Intramedullary hyperintense change on sagittal T2-weighted images (T2WI). (B) Hypertrophy of the ligamentum flavum. (C) Calcified discs. (D) Facet articular irregularity, defined as equivalent to grade 4 or 5B in the computed tomography classification. [12]
From the review of lateral radiograms, the local lordotic angle (Fig. 2A) and anteriorposterior diameter of the space available for the spinal cord (Fig. 2B) in the neutral position were evaluated at the segmental level in addition to the C2–7 lordotic angle (Fig. 2C). Local dynamic instability at the responsible segmental level was also evaluated by the difference in the distances of anteriorposterior translation of the upper vertebral body relative to the lower vertebral body in the flexed and extended positions (Fig. 2D).

Radiological assessments of degenerative changes in the cervical spine on lateral radiograms. (A) Local lordotic angle between the upper and lower vertebral body surfaces at the responsible spinal segmental level in the neutral position. (B) anteroposterior diameter of the space available for the spinal cord in the cervical spinal canal in the neutral position. (C) C2–7 lordotic angle in neutral position. (D) Dynamic segmental translation, evaluated in the flexed and extended positions: |d–d´|. a: local angle; b: space available for cord; c: C2–7 angle; d and d´: distance of anteriorposterior translation of the upper vertebral body relative to the lower vertebral body in flexed (d) and extended (d´) positions.
4. Data Analysis
The study population was divided into 2 cohorts, namely a rapid progression group and a slow progression group, depending on whether they met the definition of rapid progression. To identify and compare risk factors for rapid progression of DCM, the above-mentioned clinical and radiological variables were compared between the 2 groups; those that showed statistically significant differences were included in the logistic analysis to determine the independent risk factors for preoperative rapid progression of myelopathy and its order of relevance.
5. Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics ver. 26.0 (IBM Co., Armonk, NY, USA). Continuous variables among the clinical characteristics and radiological variables at each spinal level were compared using an unpaired ttest. Binary and nominal variables among the clinical characteristics and radiological variables were compared using Pearson chi-square test.
Logistic regression analysis was performed according to the following procedures. Independent risk factors and odds ratios (ORs) were obtained by univariate logistic regression analysis. Multivariate logistic regression analysis was performed by adding age, which was the greatest confounding factor, to the variables with large ORs to identify the variables that contributed the most to rapid DCM progression.
Data are presented as mean± standard deviation. Statistical significance was defined as p< 0.05.
RESULTS
Although 141 patients were enrolled, only 131 were included in the analyses. One patient was excluded because he had undergone revision surgery within the previous 12 months, and 9 patients were excluded because of insufficient radiological data. Meanwhile, 27 (20.6%) and 104 patients (79.4%) were categorized into the rapid and slow progression groups, respectively (Fig. 3).
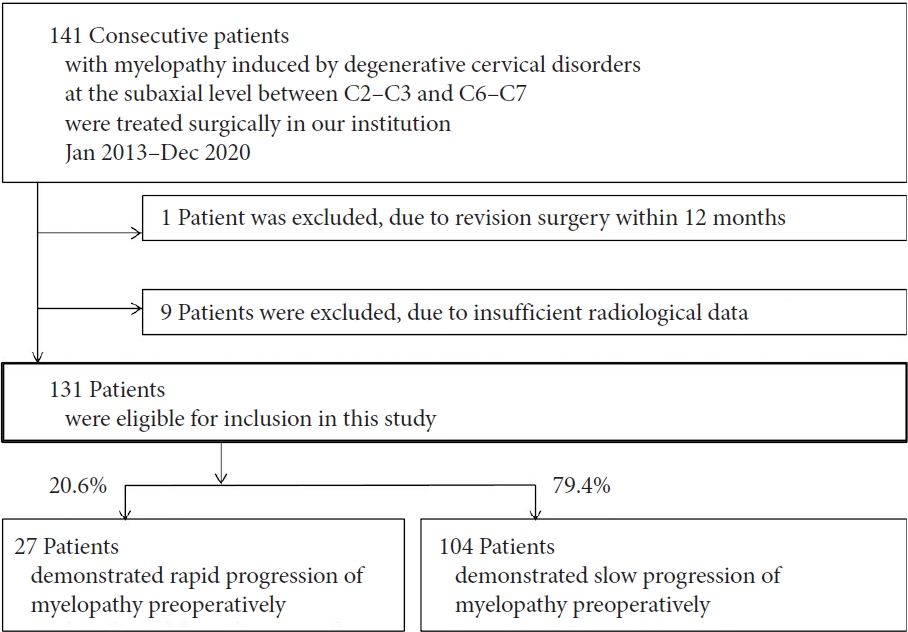
Flowchart showing the patient selection process of this study.
There were 86 men and 45 women aged 38–93 years (63.9± 12.6 years). Most patients had spondylosis (60.3%) followed by ossification of the posterior longitudinal ligament (22.1%) and cervical disc herniation (17.6%). The most common responsible segmental levels were C5–6 (36.6%) followed by C4–5 (35.1%); C2–3 were the least common (2.3%). Patients with Parkinson disease or the other movement disorders were not included.
1. Clinical Characteristics
The detailed clinical characteristics of the patients in each group are presented in Table 1. There was a significant difference between the 2 groups in terms of age (p< 0.001), hypertension (p = 0.015), diabetes (p = 0.006), history of CVE (p = 0.004), and preceding minor trauma (p= 0.008), and responsible segmental level above C4–5 (p= 0.001). The rapid progression group tended to be older and had a significantly higher incidence of these variables.

Clinical characteristics of the 2 groups (n=131)
The mean preoperative and mean postoperative JOA scores of the rapid and slow progression groups were 8.7±2.3 and 12.7± 2.4, and 12.5± 2.2 and 14.8± 2.0, respectively, which were significantly different (all p< 0.001). Meanwhile, the improvement rates in the JOA scores of the rapid and slow progression groups were 44.8%± 19.5% and 54.4%± 30.0%, respectively, which were not statistically significant.
2. Radiological Characteristics
The detailed radiological characteristics of the patients in each group are presented in Table 2. On MRI, the incidence of ligamentum flavum hypertrophy was significantly higher in the rapid progression group than in the slow progression group (p= 0.041). Meanwhile, there was no statistically significant differences in intramedullary signal changes at the responsible level or number of levels with spinal canal stenosis between the 2 groups. On CT, the incidence of facet articular irregularity was significantly higher in the rapid progression group than in the slow progression group (p< 0.001), but there was no significant difference in the presence of calcified discs between the 2 groups. Radiographic findings showed that the local lordotic angle (p= 0.037) and dynamic segmental translation (p< 0.001) were significantly higher in the rapid progression group than in the slow progression group. However, there was no significant difference in the space available for the spinal cord and C2–7 lordotic angle between the 2 groups.
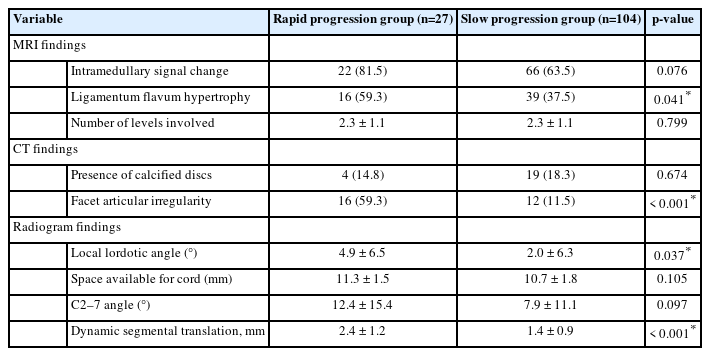
Radiological characteristics of the 2 groups (n=131)
3. Comparison of Risk Factors for Rapid Progression of DCM
Of the variables that showed statistically significant differences between the 2 groups, the 2 continuous variables, local lordotic angle and dynamic segmental translation, were converted to binary variables to homogenize the conditions of each variable and to compare them by OR; these were applied to the receiver operating characteristic analysis. The cutoff values for each variable that maximized sensitivity and specificity were then determined to be 4.5° and 1.55 mm, respectively. The 2 continuous variables were then converted into binary variables based on these cutoff values. Independent risk factors for preoperative rapid progression of myelopathy and their order of relevance were determined using logistic regression analysis (Table 3).

Logistic regression analysis for factors related to preoperative rapid neurological progression
Univariate logistic regression analysis determined facet articular irregularity (OR, 11.15; p< 0.001), dynamic segmental translation (≥ 1.6 mm) (OR, 5.744; p= 0.001), responsible segmental level above C4–5 (OR, 5.533; p= 0.003), history of CVE (OR, 4.850; p=0.007), preceding minor trauma (OR, 4.200; p=0.012), local lordotic angle (≥ 4.5°) (OR, 3.519; p= 0.005), diabetes (OR, 3.518; p= 0.008), hypertension (OR, 2.868; p= 0.017), ligamentum flavum hypertrophy (OR, 2.424; p= 0.045), and age (OR, 1.087; p= 0.001) as independent risk factors. As age was a confounding factor for many of the variables, multivariate analysis was performed by adding age to the top 3 variables based on the OR. The results revealed that facet articular irregularity was the most significant risk factor for rapid progression of DCM (OR, 6.169; p= 0.001).
DISCUSSION
This study evaluated the potential risk factors for rapid preoperative progression of DCM and their order of relevance in patients who were candidates for surgery. While many risk factors were found to be statistically significant, facet articular irregularity was the most significant risk factor.
Facet articular irregularity was reportedly observed at the responsible spinal segmental level especially in patients with rapid DCM progression [12]. The results of the current study suggest that rapid DCM progression is multifactorial, and that the finding of facet articular irregularity is potentially quite significant.
1. Rapid Progression of DCM and Associated Risk Factors
Although some studies identified the natural history or clinical predictors of slow progression in patients with CSM who were asymptomatic or treated conservatively [3-7], there have been only 3 studies that investigated rapid CSM progression. Morishita et al. [8] demonstrated that preceding minor trauma and C3–4 spinal level impairment were observed in 50% (4 of 8) and 75% (6 of 8) of cases, respectively. In contrast, comorbid sagittal instability, defined as > 3.5 mm of dynamic translation or ≥ 11° of angulation compared to the adjacent segment, was observed in only 12.5% (1 of 8) of cases. In their retrospective case–series study, Takasawa et al. [9] also demonstrated 2 risk factors based on logistic regression analysis: past history of CVE and high intramedullary signal on T2-weighted MRI. However, these studies had a major disadvantage: the responsible segmental level was not assessed by detailed neurological examination but only by assessment of intramedullary hyperintensity on T2-weighted MRI [8,9].
It is known that patients with asymptomatic spinal canal stenosis may exhibit intramedullary T2 hyperintensity of the cervical spine. In a study of 1,211 asymptomatic Japanese volunteers aged 20–79 years, Nakashima et al. [16] reported that significant spinal cord compression, intramedullary T2 hyperintensity, and flattening of the spinal cord were observed in 5.3%, 2.3%, and 3.1% of the subjects, respectively. Meanwhile, approximately one-third of patients with CSM have intramedullary hyperintensity on T2-weighted MRI [17,18], but no significant correlation has been reported between the signal intensity change and the severity of clinical symptoms [19], progression of myelopathy [6], or exacerbation of CSM in patients managed conservatively [20]. Therefore, MRI signal changes are likely to demonstrate poor reliability as predictive risk factors. Furthermore, in listing and comparing risk factors with each other, we should properly evaluate the radiological characteristics at the responsible segment level. From this perspective, the current study had the advantage of using and evaluating radiological findings of the responsible segmental level based on detailed neurological examination.
2. CT Assessment of Facet Joint Degeneration of the Cervical Spine
Although MRI is commonly used to evaluate the spinal cord in DCM, assessment of skeletal factors is also important. The discs and facet joints are crucial structures for biomechanical shifts of stress on the cervical spine as well as for mobility [21]. Rydman et al. [22] identified intervertebral disc and facet joint abnormalities as degenerative changes in their study of a CT-based grading system for CSM. In that study, disc height loss, anterior osteophytes of vertebral bodies, and endplate sclerosis were adopted as signs of disc degeneration, while joint space narrowing and the presence of irregular articular surfaces were considered to be characteristics of facet joint pathology. However, these findings generally reflect not only destabilizing factors but also stabilizing ones.
In our previous study, we attempted to subdivide cervical facet joint degeneration by considering the stage of the disease based on CT evaluation [12]. In particular, whereas previous reports had 4 categories including normal findings [23], new criteria of “articular subchondral cysts,” “articular irregularity,” “ankylosing change of the joint,” and “facet joint opening” were added, resulting in 6 classifications. With this approach, it was revealed that not only was facet articular irregularity at the responsible segmental level a remarkable finding in rapid DCM progression but that the novel CT classification is also highly reproducible, with a kappa coefficient of 0.822 for interrater concordance [12]. Therefore, the assessment of facet joint degeneration based on the novel CT grading proposes the findings of facet articular irregularity with high reproducibility.
3. Implication of Facet Articular Irregularity in Rapid DCM Progression
Because DCM is caused by age-related changes in various parts of the spine, its pathogenesis is multifactorial [1]. While the cervical facet joints play key roles not only in the stability and distribution of the axial load but also in guiding cervical motion, they are included as one of the sites that undergo age-related changes. If the changes occurring in the facet joints disrupt joint function, the facet joint pathology may cause augmentation of dynamic factors and induce DCM progression. In contrast, facet joint degeneration does not always occur synchronously with other age-related changes in the cervical spine. Lee et al. [24] showed that facet joint degeneration depends on uncovertebral joint degeneration and Modic change on MRI but not on disc or endplate degeneration, spinal stenosis, or ossification of the posterior longitudinal ligament. Therefore, facet joint degeneration should not be ignored even if other risk factors for DCM progression have been identified.
The current study found that rapid DCM progression is multifactorial, and facet articular irregularity is the most significant risk factor. There are 2 possible pathogeneses for rapid DCM progression due to facet articular irregularity. First, the multifactorial nature of rapid DCM progression suggests that microinstability of the facet joints in the presence of a pathological background, such as spinal canal stenosis, may exacerbate dynamic compression of the spinal cord.
The other hypothesis is that facet articular irregularity is a symbolic change owing to the effects of excessive motion stress. As cervical degeneration does not occur uniformly, stress from cervical spine motion is not evenly distributed and can sometimes become concentrated at 1 level. Typically, adjacent segment diseases occur after fusion surgery; however, we believe that a similar situation can occur after natural vertebral fusion or intervertebral stabilization due to advanced age. The results of this study, which showed that rapid DCM progression is more common in the elderly and at higher levels above C4–5, suggest that stabilization in the preceding middle and lower cervical spine due to age-related changes may have resulted in greater dynamic stress on the upper intervertebral joints.
We would also like to consider the significance of the difference in the frequency of facet articular irregularities between the 2 groups. Surprisingly, the rapid DCM progression group had a higher incidence of facet articular irregularity (59.3%), which was 5 times higher than that in the slow progression group. To prevent poor postoperative outcomes in patients with rapid DCM progression, surgical intervention should be performed as early as possible. Therefore, if there is a symbolic change in facet articular irregularity at the intervertebral level accompanied by spinal canal stenosis due to other factors, it may be necessary to identify the responsible spinal segmental level and consider early surgical treatment.
4. Limitations
This study had several limitations. First, it had a retrospective design with a small number of patients. Second, it is uncertain whether the responsible spinal segmental level was accurately estimated in all the cases. Third, there is a pair of facet joints at each intervertebral level that do not always have the same degree of degeneration. In the present study, we were unable to examine the differences in the clinical impact on rapid DCM progression between cases with unilateral and bilateral facet articular irregularities; further studies on this issue are warranted. Fourth, the effect of global sagittal alignment on facet joint degeneration was not evaluated in this study. Fifth, the design of this study was to statistically compare the known risk factors with additional facet articular irregularity and not to examine potential physiological mechanisms. Further studies are warranted to clarify this point.
Despite these limitations, this study demonstrated the importance and clinical usefulness of evaluating risk factors for the rapid progression of myelopathy in patients with DCM. In order to elucidate the significance of facet articular irregularities, a future study of their frequency in normal individuals and asymptomatic cases will be warranted.
CONCLUSION
This study focuses on the potential importance of facet joint pathology in patients with DCM and, for the first time, compares it with known risk factors related to rapidly progressive DCM. Facet articular irregularity is potentially the highest risk factor for rapid progression of DCM and may indicate dynamic pathophysiology in the progressive phase of myelopathy. Early surgical intervention and additional confirmation of the presence of facet articular irregularities and whether its level is consistent with the responsible spinal segmental level may also help improve surgical outcomes.
Notes
Conflict of Interest
The authors have nothing to disclose.
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contribution
Conceptualization: YT; Data curation: AO, SY, FN, IN, YP; Formal analysis: YT; Methodology: YT; Project administration: HNe; Writing - original draft: YT; Writing - review & editing: YT