Spinal Subdural Hematoma Following Meningioma Removal Operation
Article information
Abstract
Although blood contamination of cerebrospinal fluid (CSF) after an intracranial operation can occur, the development of a symptomatic spinal hematoma after craniotomy has been anecdotally reported and it is uncommon reported after a supratentorial meningioma removal operation. We report a case of spinal subdural hematoma following a supratentorial meningioma removal operation and discuss the mechanism of spinal subdural hematoma (SSDH) development. A 54-year-old woman presented with lumbago and radicular pain on both legs 4 days after a right parietooccipital craniotomy for meningioma removal. Only the straight leg raising sign was positive on neurologic examination but the magnetic resonance imaging (MRI) demonstrated a lumbosacral spinal subdural hematoma. The patient received serial lumbar tapping, after which her symptoms showed improvement.
INTRODUCTION
Spinal subdural hematoma (SSDH) is an uncommon cause of spinal cord compression and is usually associated with an trauma, lumbar puncture, haematological diseases, vascular malformations or anticoagulant therapy1,2,6,9). This condition is an unusual complication of cranial surgery2,4,6,13). The pathogenesis of spinal subdural hematoma after cranial surgery include the downward movement of blood from the cranial compartment by gravity2,3), excessive decompression of intracranial space during surgery and lowered cerebrospinal fluid (CSF) pressure by drainage2,10,11,12,13). This complication usually occurs in the setting of spinal instrumentation or coagulopathy, but a few cases occurring as a complication of cranial surgery have been reported. We report the case of a 54-years-old woman who suffered lumbago with sciatica due to a spinal subdural hematoma after supratentorial menigioma removal operation.
CASE REPORT
A 54-year-old woman presented with a several-year history of intermittent headache. There was no specific finding on physical and neurologic examination. The hematologic studies were normal. She was not on anticoagulant therapy. During her regular medical check-up, Magnetic resonance imaging (MRI) revealed an approximately 3.0×2.5 cm, well-defined, homogeneous enhancing, extra-axial mass in the right supratentorium cerebelli with loss of signal void in the right transverse sinus (Fig. 1).
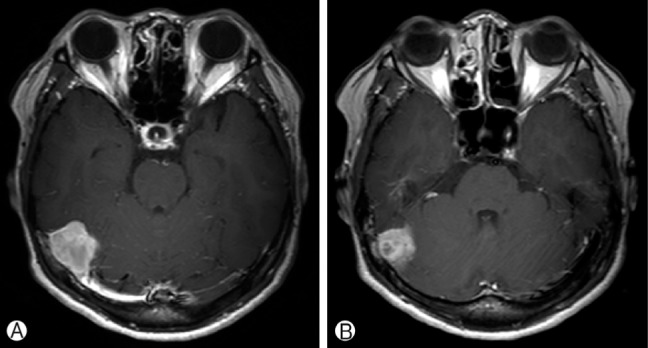
Preoperative T1-weighted contrast axial MR image showing a tumor in the right tentorium cerebellum. (A), (B).
A preoprerative angiography showed that the tumor has involved the right transverse sinus. A right parietooccipital craniotomy was performed with the patient placed in the right lateral position and 20-30° reverse Trendelenburg position. The tumor was totally removed. No noticeable bleeding during or at the end of the surgery occurred. No spinal drainage was used during the procedure. The pathological diagnosis was a fibrous meningioma.
The early postoperative period was uneventful. Postoperative CT and MRI showed a small acute infarction, small intracranial hematoma (ICH) and subdural hematoma (SDH) in the right occipital lobe and cerebellum(Fig. 2).
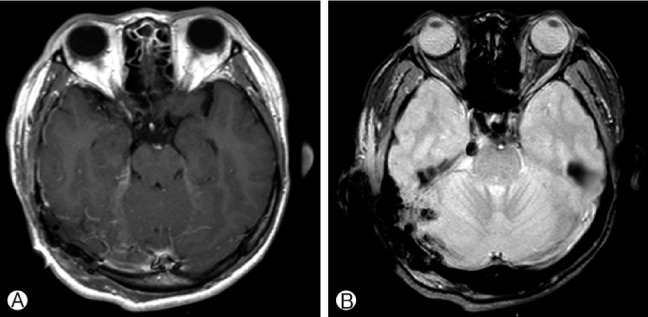
T1-weighted contrast axial (A) and Gradient echo MR image (B) at day 1 after operation, showing a small acute infarction in the right occipital lobe with small intracranial hematoma (ICH) and subdural hematoma (SDH).
She was maintained on bed rest with the head at 30° angle of elevation without mobilization. She complained of mild lumbago on the fourth postoperative day that became severe, on the fifth postoperative day was accompanied by bilateral sciatica. Her neurologic examination was normal. There knee and ankle reflexes were normal. The straight leg raising test was positive bilaterally (right 20°, left 30°). She denied having urinary retention and bowel incontinence. Coagulation tests showed no abnormalities. The symptoms persisted despite conservative treatment.
Eight days after surgery, a MRI of the lumbosacral spine obtained for the persistent lumbago showed a subacute subdural hematoma below T12 without any abnormal signal visible in the spinal cord (Fig. 3). Moreover, at the L4-S1 levels, localized hematoma formation surrounding the cauda equina was detected (Fig. 3).

MRI showing a longitudinal space occupying lesion extending from T12 to S2 in the spinal canal. A sagittal T1-weighted image showing, the homogenous lesion with a slightly higher siginal intensity relative to the spinal cord. (A) The lesion shows a homogenous signal that is isointense with the spinal cord on a T2-weighted sagittal image. (B) An axial T2-weighted image showing, the hematoma has crossed the midline. (C), (D).
Surgery was not performed in this case because the symptoms were limited to pain. Twelve days after surgery, lumbar puncture at L4-5 area was performed using a 18-gauge tapping needle. About 20 cc of dark bloody fluid was obtained. The low back pain and sciatica improved slightly after the lumbar puncture. Her symptoms redeveloped one day after the lumbar puncture. Three days after the first lumbar puncture, a second lumbar puncture was done in the same manner as before and about 5 cc of similar dark bloody fluid was drained. Almost complete pain relief was felt after the second lumbar tap. Complete pain relief was obtained two months after the onset of her lumbago and sciatica.
DISCUSSION
Factors that trigger or contribute to the development of spinal hematoma that have been reported are a trauma, coagulopathy, vascular malformations, lumbar puncture, spinal anesthesia, tumor hemorrhage, dissecting aortic aneurysm, pregnancy, immune-mediated vasculitis, vertebral surgery, arterial hypertension, and alcohol abuse1,2,6).
Spinal hematomas may migrate from a cranial lesion, a view that has been supported by many authors3,13). Lecouvet et al. explained that the propagation of blood from cranial to spinal subdural space is possible due to the presence of anatomic continuity between them5). The authors of several reports also have described the spontaneous resolution of acute intracranial subdural hematoma. When this occurs, redistribution of subdural blood is often observed with layering along dependent areas such as the tentorium3,9).
SSDH was suspected as the cause of her symptoms because she had just undergone an intracranial operation and blood contamination of the CSF is a possible consequence. MRI of the lumbosacral spine obtained for lumbago showed a subacute subdural hematoma. However, it was unclear how bleeding can occur or blood can accumulate throughout the spinal subdural area after a meningioma removal operation. So we suggested that hemorrhage due to injury of bridging vein and arachnoid membrane during operation might have been related to a progressive migration of subdural blood to the most dependent areas of the lumbosacral region under the influence of gravity. Also, we believe that the pathogensis of the present patient's condition was basically the movement of blood from the intracranial operative site into the spinal subdural space via the CSF circulation system with the added effect of gravity due to the lateral positioning and postoperative ambulation of the patient.
In most cases, it was reported that SSDH case's symptom after cranial surgery is milder than SSDH case's symptom due to bleeding tendency and is usually improved within 2 weeks4,6,9). Severe symptoms or clinical worsening are observed, surgical intervention should be applied. Some authors have suggested that spinal subdural hematoma confined to the lumbar level could be successfully managed by percutaneous drainage7,8). In this case, twelve days after surgery, we performed serial lumbar tapping to relieve the pain. We hypothesized that small amount of continuous bleeding at operative site can accumulate throughout the spinal subdural area. So we thought that a small quantity of the old blood aspirated from the main lesional (L4-5) site would provide relief of pain due to its decompressive effect between the dura matter and arachnoid membrane junction. Also, we could not appiled the lumbar drainage by catheter, because lumbar drainage catheter may aggravate the compression of the cauda eqiuna and further irritate it.
CONCLUSION
Accordingly, in patients with intracranial cranial surgery complaining of lower back pain and radicular pain in both legs, lumbosacral MRI examination should be performed. Serial lumbar tapping may be indicated for patients with lumbago and radicular pain on both legs due to spinal subdural hematoma following a supratentorial meningioma removal operation as was seen in the present case.