Severe Obesity Is an Independent Risk Factor of Early Readmission and Nonhome Discharge After Cervical Disc Replacement
Article information

Abstract
Objective
Despite growing interest in cervical disc replacement (CDR) for conditions such as cervical radiculopathy, limited data exists describing the impact of obesity on early postoperative outcomes and complications. These data are especially important as nearly half of the adult population in the United States is expected to become obese (body mass index [BMI] ≥ 30 kg/m2) by 2030. The goal of this study was to compare the demographics, perioperative variables, and complication rates following CDR.
Methods
The 2005–2020 American College of Surgeons National Surgical Quality Improvement Program datasets were queried for patients who underwent primary 1- or 2-level CDR. Patients were divided into 3 cohorts: Nonobese (BMI: 18.5–29.9 kg/m2), Obese class-I (BMI: 30–34.9 kg/m2), Obese class-II/III (BMI ≥ 35 kg/m2). Morbidity was defined as the presence of any complication within 30 days postoperatively. Rates of 30-day readmission, reoperation, morbidity, individual complications, length of stay, frequency of nonhome discharge disposition were collected.
Results
A total of 5,397 patients were included for analysis: 3,130 were nonobese, 1,348 were obese class I, and 919 were obese class II/III. There were more 2-level CDRs performed in the class II/III cohort compared to the nonobese group (25.7% vs. 21.5%, respectively; p < 0.05). Class-II/III had more nonhome discharges than class I and nonobese (2.1% vs. 0.5% vs. 0.7%, respectively; p < 0.001). Readmission rates differed as well (nonobese: 0.5%, class I: 1.1%, class II/III: 2.1%; p < 0.001) with pairwise significance between class II/II and nonobese. Class II/III obesity was an independent risk factor for both readmission (odds ratio [OR], 3.32; p = 0.002) and nonhome discharge (OR, 2.51; p = 0.02). Neither 30-day reoperation nor morbidity rates demonstrated significance. No mortalities were reported.
Conclusion
Although obese class-II/III were risk factors for 30-day readmission and nonhome discharge, there was no significant difference in reoperation rates or morbidity. CDR procedures can continue to be safely preformed independent of obesity status.
INTRODUCTION
Patients with cervical myelopathy and radiculopathy have been classically treated with anterior cervical discectomy and fusion (ACDF) after failure of conservative measures [1-3]. ACDF has shown admirable efficacy over the years, but the procedure is associated with numerous complications, including pseudoarthrosis, adjacent segment disease, dysphagia, and loss of cervical range of motion as well as inherent risks of harvesting bone graft [1,4]. In recent decades, an alternative method, cervical disc replacement (CDR), has gained popularity due to its potential to reduce the postoperative risks associated with ACDF. Unlike ACDF, CDR preserves range of motion, decreases adjacent segment disease, and does not require a plating graft. CDR has also shown comparable efficacy, safety, and overall outcomes to ACDF [5]. However, despite the growing body of literature supporting CDR, there has been little investigation into the impact of obesity on early postoperative outcomes and complications of this procedure. This is a significant knowledge gap, given that obesity is a growing public health crisis in America with 49% of the United States (US) adults predicted to be obese by 2030, and the prevalence of severe obesity (body mass index [BMI] ≥ 35 kg/m2) is expected to spike to 24.2% in the US adults within the same timeframe [6].
Obesity is a well-known risk factor for numerous postsurgical complications in spine surgery, including venous thromboembolism, surgical site infection, and blood loss, and severe obesity has been shown to correlate with a higher risk of early complications [7,8]. Obese patients may be especially prone to poorer outcomes in specifically anterior cervical surgery as different cardiopulmonary risks, difficult approaches, and retraction in obese patients have previously described in these surgeries even compared to lumbar spine surgery. So, while there have been previous studies describing obesity as a risk factor for early postoperative complications in ACDF [9], to our knowledge, to date, no study has described these outcomes in CDR. ACDF and CDR are technically very different surgeries and impact biomechanics of the spine in different ways. Obesity may be even more crucial to understand in CDR than ACDF since the replaced intervertebral disc has a very different function than a functionally temporary graft used in ACDF procedures. The rising relevance of both CDR and obesity presents a crucial need for further inquiry. Therefore, the purpose of this study was to (1) investigate perioperative complication profiles, readmission rates, and mortality following CDR for obese patients, and (2) outline patient demographic variables in obese patients that may be associated with higher complications.
MATERIALS AND METHODS
1. Study Population
Data was collected via the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. The NSQIP database is a validated, multicenter, prospective database designed to measure quality of surgical care and track early patient outcomes [10,11]. Patients undergoing primary 1 or 2 level CDR procedures between 2005 and 2020 were queried for this analysis. This was extracted via current procedural terminology (CPT) codes 22856 and 22858 for CDR. Patients undergoing revision CDR (22861) and removal CDR (22864) were excluded. ACDF (22551, CPT2552), anterior cervical fusion (22554, 22585), posterior cervical fusion (22590, 22600, 22614), cervical laminoplasty (63050) procedures were also excluded. Consistent with prior methods, emergent/non-elective cases, fractures, and infection cases were all excluded from the NSQIP query.
Following data was pulled from the NSQIP database. Patients with missing demographics were excluded.
(1) Preoperative data: surgical setting (outpatient [length of stay< 24 hours], inpatient [length of stay≥ 24 hours]), patient demographics (age, BMI, sex, race, ethnicity, functional status, smoking status, American Society of Anesthesiologists [ASA] physical status classification, comorbidities [i.e., diabetes, congestive heart failure, chronic obstructive pulmonary disease, bleeding disorders], laboratory values [creatine, hematocrit, white blood, and platelet cell count]).
(2) Operative data: type of surgery, number of levels, operation time, and length of stay.
(3) Postoperative data: discharge disposition (home, nonhome), 30-day morbidity (complications including wound infections, urinary tract infection, pneumonia, sepsis, unplanned intubation, renal insufficiency/failure, stroke, myocardial infarction, thrombosis/embolism, transfusions), readmission, and reoperation.
BMI was the primary independent variable of interest. To fully appreciate the effect of BMI on the patient’s surgical risk profile, patients were categorized into nonobese (BMI: 18.5–29.9 kg/m2), obese class I (BMI: 30–34.9 kg/m2), and obese class II/III (BMI≥ 35 kg/m2) in accordance with the World Health Organization BMI classification [12]. Severe obesity can be defined as patients obese class II/III. Any patients with BMI< 18.5 kg/m2 were excluded.
2. Statistical Analysis
Across BMI groups, demographic factors and postoperative outcomes for categorical variables were compared with Pearson chi-square test or Fisher exact test when applicable. Analysis of variance and Kruskal-Wallis tests were used for continuous normally and nonnormally distributed variables respectively. Post hoc, pairwise t-tests were conducted if there was a significant difference among the 3 cohorts. Univariate logistic regression and multivariable logistic regressions were then carried out to investigate independent predictors of morbidity, reoperation, readmission, and nonhome discharge disposition. Significance was defined with a p-value ≤ 0.05. All analyses were performed using IBM SPSS Statistics ver. 25.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Demographics
A total of 5,397 patients were included in this analysis; 3,130 (58%) were nonobese, 1,348 (25%) were obese class I, and 919 (17%) were obese class II/III (Table 1). Nonobese patients had significantly lower rates of diabetes (class I: 5%, class II: 11.4%, class III: 18.2%, p<0.001), dyspnea (1.3%, 1.5%, 3.9%, p<0.001), hypertension (19.6%, 32.8%, 44.3%, p < 0.001), and bleeding disorder (0.2%, 0.6%, 0.9%, p= 0.012) compared to obese class I and obese class II/III patients. The percentage of patients with ASA physical status classification grade ≥ III was also significantly lower for nonobese patients compared to obese patients (14.5%, 25.1%, 49.9%, p<0.001).

Demographical and clinical characteristics (n=5,397)
2. Perioperative and 30-Day Outcomes
A greater percentage of obese class II/III underwent 2-level CDR procedures compared to nonobese patients (25.7% vs. 21.5%, p= 0.021). While there were no differences in surgical complications among the 3 groups, the percent of patients with a nonhome discharge disposition (0.5%, 0.7%, 2.1%, p<0.001) and 30-day readmission (0.5%, 1.1%, 2.1%, p<0.001) were significantly higher for obese patients compared to nonobese patients. While not statistically significant, there was a trend towards higher rates of reoperations for obese patients (0.4%, 0.5%, 1%, p<0.094). Length of stay and total operation time were not significantly different between the groups (p < 0.05 for both) (Table 2).

30-day outcomes and perioperative variables (n=5,397)
3. 30-Day Readmission
On a univariate analysis, age (odds ratio [OR], 1.04; p= 0.005), BMI as a continuous variable (OR, 1.06; p<0.001), obese class I (OR, 2.06; p= 0.042), obese class II/III (OR, 3.87; p<0.001), Hispanic ethnicity (OR, 3.02; p<0.021), dependent functional status (OR, 9.45; p= 0.003), ASA physical status classification grade ≥ III (OR, 2.54; p= 0.001) were all significant predictors of 30- day readmission. Comorbidities including dyspnea, hypertension, and dialysis all also had significantly higher odds of readmission (Supplementary Table 1). Outpatient surgery setting was a protective factor for readmission (OR, 0.5; p= 0.015). On multivariable analysis, BMI as a continuous variable (OR, 1.06; p<0.001) and obese class II/III (OR, 3.32; p= 0.002) both remained significant predictors of readmission. Outpatient surgery setting remained a protective factor for readmission (OR, 0.55; p= 0.049) (Table 3).

Multivariable regression: 30-day readmission
4. Nonhome Discharge Disposition
On a univariate analysis, age (OR, 1.06; p<0.001), BMI as a continuous variable (OR, 1.06; p<0.001), obese class II/III (OR, 4.12; p<0.001), Hispanic ethnicity (OR, 5.32; p<0.001), dependent functional status (OR, 10.99; p<0.001), ASA physical status classification grade ≥ III (OR, 4.85; p<0.001) were all significant predictors of nonhome discharge disposition. Comorbidities including dyspnea, hypertension, and dialysis all also had significantly higher odds of nonhome discharge. Outpatient surgery setting was a protective factor for nonhome discharge (OR, 0.3; p<0.001) (Supplementary Table 1). On multivariable analysis, BMI as a continuous variable lost significance, but obese class II/III (OR, 2.51; p= 0.027) remained a significant independent predictor of nonhome discharge. Hispanic ethnicity (OR, 6.76; p<0.001) and ASA physical status classification grade ≥ III (OR, 3.37; p= 0.001) both remained significant predictors. Outpatient surgery setting remained a protective factor for nonhome discharge (OR, 0.31; p= 0.002) (Table 4).

Multivariable regression: nonhome discharge disposition
5. 30-Day Morbidity
On univariate analysis, BMI as a continuous variable (OR, 1.04; p= 0.01) and ASA physical status classification grade ≥ III (OR, 2.23; p= 0.004) were significant predictors of 30-day morbidity. Obesity class II/III, though not significant, did have an elevated odds ratio (OR, 1.78; p= 0.093). Comorbidities including diabetes and chronic steroid use also had significantly higher odds of morbidity. Outpatient surgery setting was a protective factor for morbidity (OR, 0.48; p= 0.007) (Supplementary Table 1). On multivariable analysis, BMI as a continuous variable lost significance as a predictor of morbidity. Chronic steroid use (OR, 4.26; p= 0.003) and elevated perioperative white blood cell count (OR, 4.06; p<0.001) were significant independent predictors of morbidity. Outpatient surgery setting remained a protective factor for morbidity (OR, 0.49; p= 0.019) (Table 5).

Multivariable regression: 30-day morbidity
6. 30-Day Reoperation
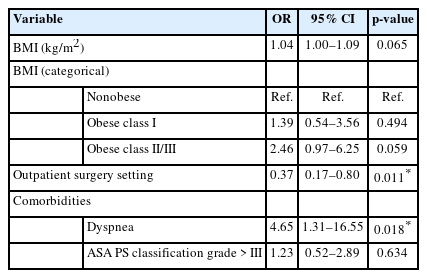
On univariate analysis, BMI as a continuous variable (OR, 1.05; p= 0.025), obese class II/III (OR, 2.57; p= 0.033) were significant predictors of 30-day reoperation. Comorbidities including dyspnea and smoking status also had significantly higher odds of reoperation. Outpatient surgery setting was a protective factor for reoperation (OR, 0.4; p= 0.019) (Supplementary Table 1). On multivariable analysis, though the odds ratios were still elevated, BMI as a continuous variable and obese class II/III both lost statistical significance in prediction of reoperation. Dyspnea and smoking status remained significant predictors. Outpatient surgery setting remained a protective factor for reoperation (OR, 0.37; p= 0.011) (Table 6).
Multivariable regression: 30-day reoperation
DISCUSSION
As the rates of obesity continue to rise, there is high demand to understand its effect on surgical outcomes. While there exists strong evidence broadly supporting obesity as a risk factor for various spinal pathologies, there remains relatively little exploring the effect of obesity clinical outcomes of CDR. In the present study we looked to investigate if obesity is associated with a higher risk for early postoperative complications and outcomes following CDR. Utilizing the ACS-NSQIP database, we have shown that obesity was associated with an independent risk for 30-day readmission and nonhome discharge disposition. However, obesity was not significantly associated with the risk of postoperative morbidity outcomes.
Obesity was found to be a risk factor for 30-day readmission following CDR. When categorized, severe obesity (class II/III) was associated with a 3.32-fold increased 30-day readmission risk. Understanding risks of readmission has recently become of great interest. These unplanned readmissions for Medicare patients alone cost the federal government an estimated $17.4 billion annually, and so it is a point of focus to improve healthcare efficiency and affordability [13,14]. Obesity as a risk factor for readmission risk has not yet been fully understood. While obesity has been shown as a risk for readmission in various surgical specialties [15-18], other analyses have found it as an insignificant factor [19]. Here we have found that within the setting CDR, obesity does increased risk of readmission. 30-day reoperation rates were also analyzed. While obesity was not significantly associated with increased rates of reoperation, it is worth noting that with each class of obesity, the percentage of patients reoperated on increased. Obesity has been long shown in spine surgery to increase rates of operative complications [7,8,20,21]. Jiang et al. [21] conducted a meta-analysis of 32 studies and almost 100,000 patients looking at rates of complications amongst obese patients undergoing spine surgery. They found that various complications including surgical site infection, venous thromboembolism, mortality, revision rate, and blood loss were all increased amongst obese patients. Readmission and reoperation risks are highly associated with operative or postoperative complications [17,22]. The increased risk of complications likely yields the outcomes of increased readmissions amongst obese patients. In an effort to improve patient quality of life and increase health care efficiency, further understanding how obesity mediates this increased risk of readmission and potential reoperation could be helpful. Obesity was also found as an independent risk factor for nonhome discharge disposition following CDR. In the multivariable analysis, obesity as a continuous variable was not associated with an increased risk for nonhome discharge but as a categorical variable, obesity class II/III was. In a similar way, it is likely obese patients have a higher comorbidity burden which is a significant factor in deciding the need for a nonhome discharge disposition.
Our analysis found various comorbidities associated with obesity that are in line with existing literature. Obesity was significantly associated with diabetes, dyspnea, hypertension, and bleeding disorders. It is also worth noting that when stratifying obesity by BMI, higher classes of obesity had even greater risks for these comorbidities. These findings are well in alignment with existing literature regarding the risks associated with obesity [23,24] which provides some additional external validation of the data presented here. These various comorbidities were also associated with various complications. ASA physical status classification grade ≥ III was an independent risk factor for nonhome disposition and was a significant risk factor for readmission and morbidity on the univariate analysis. Individual comorbidities were also analyzed. Dyspnea for example was a significant independent risk factor for 30-day reoperation. In the univariate analysis, various other comorbidities were associated with the worse outcomes investigated: dyspnea (readmission, nonhome discharge reoperation), hypertension (readmission, nonhome discharge), dialysis (readmission, nonhome discharge), diabetes (morbidity). So, while is possible that these other comorbidities play an independent role, obesity was the only one constantly measure remaining significant across all the outcome measures in the multivariable analysis. In fact, these likely mediate the elevated risk of readmission and nonhome discharge seen in obese patients. In a similar way, we show that patients that underwent surgeries in ambulatory settings had decreased odds of readmission, reoperation, morbidity, and nonhome discharge. Patients whose surgeries are done in ambulatory centers tend to have lower comorbidity burdens, and thus we would expect them to be at lower risk for these complications [25].
Another potential explanation for the poorer outcomes found here independently associated with obesity following CDR is the increased surgical complexity associated with a larger body habitus. Previous studies have described longer set up times with more difficult patient positioning, the necessity for larger incisions, and more difficult retraction associated with more subcutaneous fat in spine surgery [26-28]. Rosenfeld et al. [29] additionally reported that preoperative and intraoperative radiographs were less accurate in obese patients and potentially required higher radiation doses, increasing the surgical difficulty in those cases. Anterior cervical surgery specifically may be additionally more challenging in patients with shorter necks and large neck circumferences. In ACDF surgeries, Qi et al. [30] reported that neck circumference, neck length, and associated increased BMI were all risk factors for complications. The increased rates of readmission and nonhome discharge disposition for obese class II/III patients following CDR therefore may be partially explained by the increasing difficulty of surgeries in this population.
This study did have several limitations worth noting. Despite the large initial sample size of patients included in this analysis, the rates of various complications were very low. These complications may be too infrequent to elucidate significant differences without much larger sample sizes. This study is also prone to various limitations associated with the retrospective methodology employed. NSQIP is a prospective database that we have retrospectively reviewed. This methodology can lead to potential for selection bias in the analysis. Similarly, this study is prone to limitations associated with the usage of the NSQIP database itself. The database was curated from certain participating centers, which may not result in a representative sample of the whole population of patients undergoing CDR. Additionally, the differences in patient care are inevitable with such a database, and with such small rates of complications, such variances can affect the reproducibility of the data. Additionally, other comorbidities and complications were not recorded in this database, and these other factors may be important in assessing the risk of complications for obesity in CDR. Despite these limitations, we believe that the large sample size and quality data from NSQIP make the findings presented here valid and applicable for CDR. We additionally acknowledge that obesity can be part of a broader spectrum of metabolic disease so further research may be necessary to isolate obesity as an independent risk factor or analyze metabolic syndrome’s impact on early outcomes following CDR.
CONCLUSION
Obesity is an epidemic and growing public health concern that costs the US an estimated $209.7 billion dollars annually [31]. As such, it becomes increasingly important to truly understand the effects and risks on medical care and surgical procedures. Although the negative impacts of obesity have been reported as a general surgical risk factor for spine surgery [32], to our knowledge, our study is among the first to analyze its risk for early postoperative complications following CDR. In this analysis of over 5,000 patients, obesity was found to be a risk factor for readmission and nonhome discharge but was not associated with morbidity in these patients. Based on this analysis, we believe patients can safely undergo CDR without a significantly increased risk of complications, but appropriate counseling is still necessary.
Supplementary Material
Supplementary Table 1 can be found via https://doi.org/10.14245/ns.2346442.221.
Univariate regression
Notes
Conflict of Interest
The authors have nothing to disclose.
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contribution
Conceptualization: TS, DS, JD, SI, SQ; Data curation: DS, IA, OM, EZ, KA; Formal analysis: TS, DS, IA, OM, EZ, KA; Methodology: TS; Project administration: JD, SI; Writing - original draft: TS, DS; Writing - review & editing: TS, PS, TA, JS, SD, JD, SI, SQ.