Ligamentum Flavum Cyst of Lumbar Spine: A Case Report and Literature Review
Article information
Abstract
Ligamentum flavum cysts have rarely been reported and known to be the uncommon cause of spinal compression and radiculopathy. A 63-year-old man presented right sciatica lasting for 1 month. Lumbar computerized tomography and magnetic resonance imaging demonstrated an extradural cystic mass adjacent to the L5-S1 facet joints. Partial hemilaminectomy and flavectomy at the L5-S1 space were performed, and then the cystic mass was excised. Histopathology confirmed a connective tissue cyst, which is consistent with the ligamentum flavum. Microscopic examination of the cyst wall revealed that it is closely packed collagen fibril. The symptom of patient was improved after surgery. Because of rarity of ligamentum flavum cysts and nonspecific clinical and radiologic findings, the preoperative diagnosis is not easy. The histologic features of ligamentum flavum cysts are distinct from other cystic lesion of lumbar spine. This study presents a case and literature review of ligamentum flavum cyst. We summarize the pathophysiology, occurrence, differential diagnosis of rare ligamentum flavum cyst, especially on lumbar spine.
INTRODUCTION
After first report by Moiel et al. in 196719), cysts of the ligamentum flavum have rarely been reported and they are known to be an uncommon cause of spinal compression and radiculopathy22). Ligamentum flavum cyst is one of the juxtafacet cysts. Kao et al.15) and Rhoton et al.21) first used the term "juxtafacet cyst" in 1974 to describe synovial and ganglion cysts that are adjacent to the facet joints or arise from or grow into the ligamentum flavum. Some authors classified juxtafacet cysts into three types by location: facet cyst, flavum cyst, and posterior longitudinal ligament (PLL) cyst1). Histologically, juxtafacet cysts are classified into the two types: a synovial cyst with a synovial lining membrane and a ganglion cyst with no synovial lining membrane. In 1995, Chimento et al.9) reported that almost all cysts of the ligamentum flavum and PLL are ganglion cysts. But the pathophysiology of ligamentum flavum cysts has not yet been fully elucidated.
In current report, the authors present one case of ligamentum flavum cyst on lumbar spine and summarize their pathophysiology, occurrence, differential diagnosis, on the reported articles.
CASE REPORT
A 63-year-old man presented with right sciatica of 1 month's duration. He also suffered from low back pain and hypoesthesia of the posterior aspect of the right lower extremity. On neurological examination, he had no motor paresis, intermittent claudication or urinary incontinence. We performed computerized tomography (CT) and magnetic resonance imaging (MRI) to evaluate the spinal lesion.
CT imaging of the lumbosacral spine showed some degenerative marginal osteophytes and degenerative facet arthropathy in the lumbar spine. Axial CT on the L5/S1 level showed ruptured disc-like material, but it had an unusual isodensity mass within air density. And CT-myelogram showed an extradural cystic mass, located in the dorsal area of the right inferior facet and the dorsolateral area of the right S1 root and thecal sac (Fig. 1). MRI revealed a 1.2 cm sized cystic lesion rather than a disc, compressing the thecal sac and right S1 nerve root in the right L5-S1 facet joint. The cystic lesion showed isointensity mass on T1 and T2-weighted images. And it seemed to originate from the facet or ligament flavum(Fig. 2). Based on these radiologic finding and clinical symptoms, we diagnosed this lesion as a synovial cyst and performed an operation.
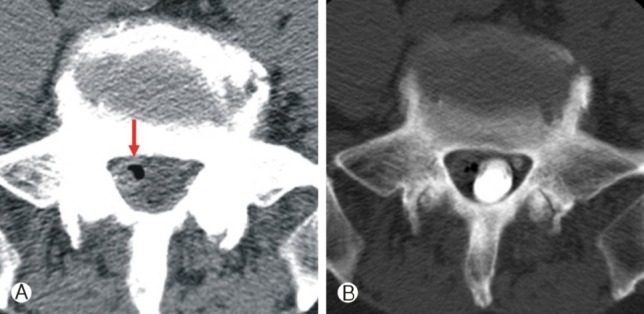
Lumbar axial computerized tomography (CT) on L5/S1 level showing the ruptured disc-like material, but is unsual isodensity mass within air density (A). CT after myelogram showing the extradural mass, locating ventrolateral area of right S1 root (B).
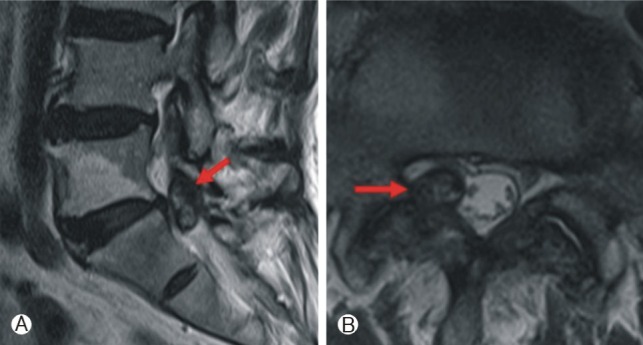
T2-weighted sagittal magnetic resonance imaging (MRI) showing that the 1.2 cm sized cystic mass was disconnected the L5-S1 intervertebral disc and seemed to originate from facet or ligament flavum(A). T2-weighted axial MRI demonstrating the isointense mass. In addition, it compressing the thecal sac and right S1 nerve root (B).
The patient was placed under general anesthesia in the prone position. A longitudinal midline incision with exposure of the L5-S1 junction was made. As we carried out partial hemilaminectomy on the right L5 lamina, we found moderate thickening of the capsule of the apophyseal joint and thickened ligamentum flavum. The mass was originated from ligament flavum and contained yellow cystic fluid. The mass compressed the thecal sac and tightly adherent to dura. While the cyst and the ligament were adherent to the dura, there was no communication with the subarachnoid space or connection with the apophyseal joint (Fig. 3). The right S1 nerve root was compressed and pushed laterally by the cyst, and after removal of cyst, nerve root was completely released. There were tight adhesions to dura around the cyst, so dural tearing and CSF leakage occurred during the mass removal. We sealed the dural tear site using a Tachocomb, and performed lumbar drainage. In addition, we could not find a protruding disc or any other mass compressing the root.

Intraoperative finding. The mass was originated from ligament flavum and contained cystic fluid. The mass was compressing the thecal sac and tightly adherent to dura.
Histopathology confirmed a connective tissue cyst consistent with a cyst of the ligamentum flavum. Histopathologic microscopic examination of the cyst wall revealed that this was closely packed collagen fibrils without a synovial lining (Fig. 4). There was no nerve tissue in the wall and it was not covered by epithelium. The patient had relief from the sciatica and hypoesthesia after surgery completely. The lumbar drain was removed after one week and the patient was discharged free of pain.
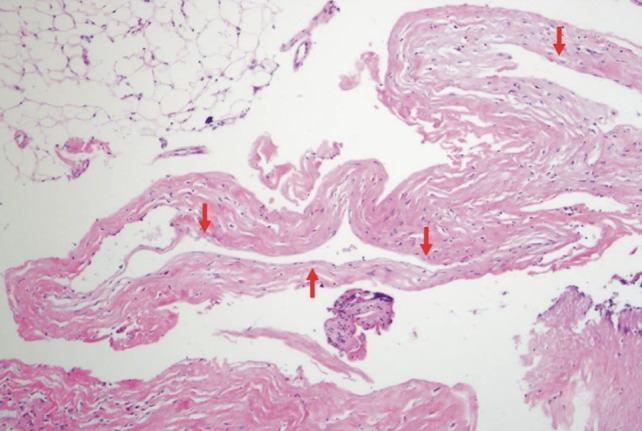
Photomicrograph of the surgical specimen showing cyst formation. The cyst wall (arrows) consists of fibrotic connective tissue without synovial lining (×200, H&E)
DISCUSSION
Anatomically, the ligamentum flavum is attached above and below to the lamina and laterally to the capsule of the articular facets. The ligament turns dorsally in the intervertebral foramen and is fused with the capsule on the lateral surface of the superior articular process in the lumbar spine.
The pathogenesis of ligamentum flavum cysts is not yet fully elucidated, but it has proposed that continuous stress to the ligamentum flavum due to minor chronic trauma such as in spondylolisthesis and degenerative disc disease may predispose a patient to developing this cyst8).
Incidence of intraspinal ligamentum flavum cysts is rare and they occur frequently in the lower lumbar region24). Ligamentum flavum cysts in the lumbar spine occur commonly at L4-5 level because this level is the most mobile segment. In the cervical spine, only a few cases have been reported. With article searching about ligamentum flavum cysts, we found the 66 cases of ligament flavum cysts occurring in the lumbar spine. The frequency at lumbar spine of ligamentum flavum cyst was as follows: L4-5 (56%), L5-S1 (23%), L3-4 (20%), L2-3 (1%) level (Table 1).

Reported 66 cases of ligament flavum cysts occurring in the lumbar spine
There are no specific clinical symptoms for ligamentum flavum cyst. Symptomatic ligamentum flavum cysts usually present with radiculopathy and can mimic symptoms of intervertebral disc herniation11). They can be found incidentally14). The clinical symptoms of ligamentum flavum cysts are as follows: 97% of patients complained of radicular pain, 55% sensory changes, 39% motor deficit, 33% positive Lasèque sign, and 18% abnormal reflexes. Our patient had low back pain and severe radicular pain, and no motor deficit.
In the past, hypertrophy of the ligamentum flavum was considered as a cause of lumbar nerve root compression in pathologic conditions like spondylosis. With increasing understanding of degenerative diseases of the spine, a new concept of the ligamentum flavum as a cause of pathologic conditions has been established. Besides common degenerative changes in connective tissues like hyaline or mucoid changes, more extensive degenerative changes like necrosis, fibrosis, calcification and cyst formation are related to the development of ligamentum flavum cysts20).
Ligamentum flavum cysts must be differentiated from the synovial or ganglion cysts which are common lesions occurring in the facet joints. Kao et al. and Rhoton et al.15) distinguished these two lesions according to several factors. Synovial cysts arise from the facet joints and remain outside the ligamentum flavum. Characteristically, they have a synovial lining membrane. They are continuous with the joint space and are lined by pseudostratified columnar epithelium, and are filled with clear and xanthochromic fluid. In contrast, ganglion cysts have no synovial lining membrane and do not communicate with the facet joint, and contain gelatinous material. Both are usually found at the L4-5 level38). So we think that this is a case of synovial cyst from facet joint.
The differential diagnosis of cystic lesions involving the ligamentum flavum includes granuloma, intraligamentous amyloid deposition, ossification, myxomatous degeneration and hematoma, perineural cyst, intraspinal dermoid cyst, neurofibroma, hydatid cysts or cysticercosis5,15).
Radiological differentiation of ligament flavum cysts is difficult. Plain X-rays mostly show only degenerative changes. Myelogram showed the intraspinal extradural masses compressing the nerve root sleeve4). Because the radiologic features are nonspecific, differentiation from other intraspinal cysts is very difficult.
Recently MRI has been widely used for diagnosis of juxtafacet cyst, but no specific features have been reported. Generally, the cysts have a variable signal on T1-wighted and a hyperintense T2-weighted images26). In our patient, the ligamentum flavum cyst was isodense with air on CT, isointense in T1 and T2-weighted MRI, and there was no communication with the spinal facet joint. Ligament flavum cyst often occur with intraluminal hemorrhage, and sometimes air or gas forming ligamentum flavum cysts have been reported.
Conservative therapy has not shown successful results. Percutaneous steroid injection of the facet and juxta-facet cysts also has effect on short term7). Percutaneous aspiration of cyst has not been effective. Surgical excision is the treatment of choice. The goal of surgery is spinal decompression and resection of the cyst and the affected ligamentum flavum. If complete excision of the cyst is performed, recurrence is unlikely2). The presence of adhesions to the dura is known to be the main factor in incomplete resection and recurrence18). The neurological outcome after surgical treatment is good, including the improvement of pain8).
CONCLUSION
Ligamentum flavum cyst is a rare cause of spinal compression and radiculopathy. Because of its rarity and the nonspecific clinical and radiologic findings, the preoperative diagnosis is not easy. It can be distinguished from other juxtafacet cysts by several findings. We report the ligamentum flavum cyst on lumbar spine which was successfully treated by surgical excision and literature review.