Iatrogenic Intraspinal Epidermoid Cyst
Article information
Abstract
Epidermoid cyst is generally regarded as congenital disease, and commonly related to other congenital spinal anomalies. However, it also develops iatrogenically. We report one rare case of epidermoid cyst that we experineced among intradural extramedullary tumors. A 21-year-old female patient was admitted to the hospital due to low back pain with radiating pain into a right lower extremity that initiated about a month ago. She complained sensory lose and motor weakness (grade 4+) on her right extremity as well as urinary dysfunction and sphincter dysfunction. She had a lumbar puncture three times due to Pneumococcal meningitis when she was 13 years old. The well-circumscribed intradural extramedullary mass of 1.8×1.6×4 cm size was found on the L4-5 in a magnetic resonance image. Gross total tumor removal was garried out after the total laminectomy L5 and partial laminectomy L4. The tumor mass was gray-colored and so fragile that it was easy to be removed. The histological diagnosis confirmed epidermoid cyst without malignancy. After the operation, the patient progressively showed remarkable neurological recovery. In this case, the cause of epidermoid cyst is considered iatrogenic concerning history of several times of lumbar puncture as meningitis.
INTRODUCTION
Epidermoid cyst, also called "pearly tumor" because of the smooth, glistening, white capsule, is a rare, and slow growing benign tumor, which represents less than 1% of all intraspinal tumors2,10). Most intraspinal epidermoid tumors are intradural extramedullary and their origin may be congenital or acquired. Congenital epidermoid tumors may develop from displaced cutaneous ectoderm during neural tube formation9), while the common cause of an acquired epidermoid tumor is implantation of epidermal tissue in the subdural space during surgery or lumbar puncture3,9,12).
We report one rare case of an iatrogenic epidermoid cyst occurring intradural extramedullary portion.
CASE REPORT
A 21-year-old female patient was admitted to the hospital due to low back pain radiating into the right lower extremity that initiated approximately one month ago. There was no obvious swelling or deformity and no midline tenderness on palpation of the spine. She complained of sensory loss and motor weakness (grade 4+) in her right lower extremity, as well as urinary and sphincter dysfunction. Severe limitation was checked during the straight leg raising (SLR) test as 45° on the patient's right side. There were no pathologic reflexes.
There was no significant abnormality at birth, nor any notable problems except three lumbar punctures due to pneumococcal meningitis when she was 13 years old. The type of needle used was not documented. No abnormality was found in the skin over the lumbosacral region.
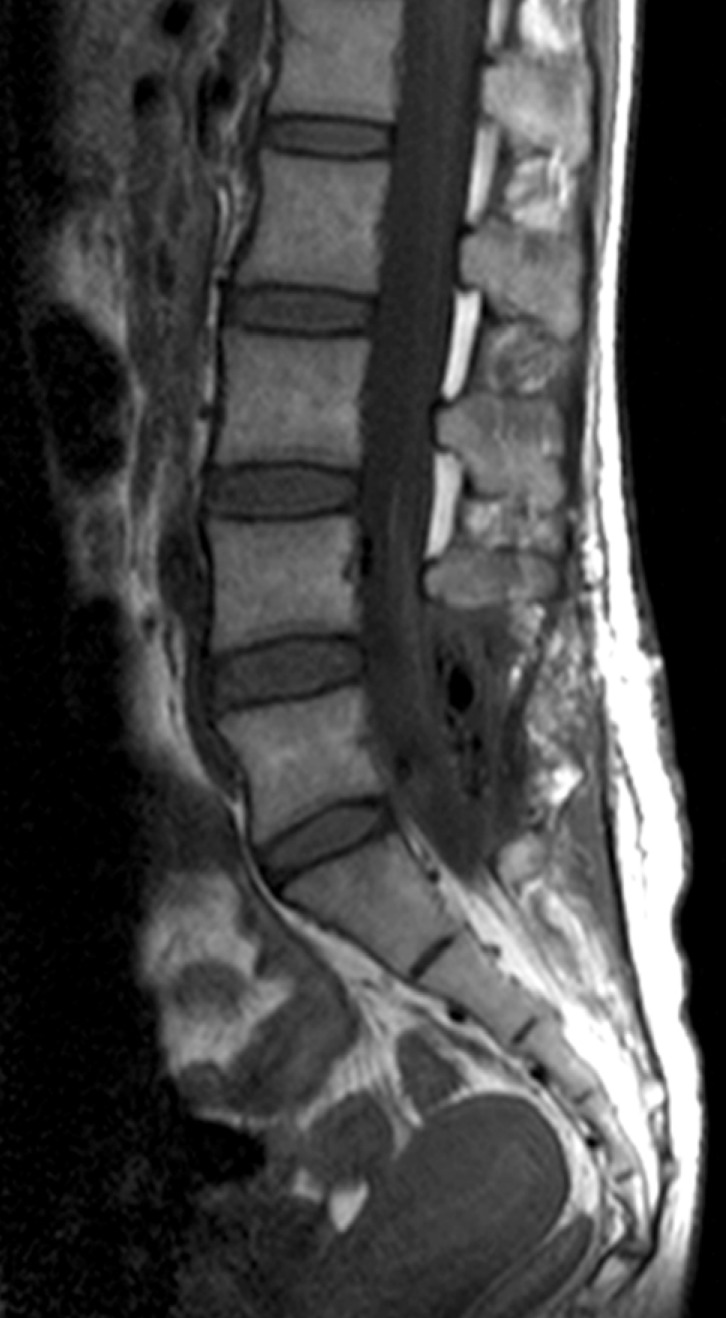
Plain radiographs of her lumbosacral spine were normal. Magnetic resonance imaging (MRI) of the spine demonstrated a well circumscribed intradural extramedullary mass of 1.8×1.6×4 cm size at the L4-5 level. In a T1-weighted image, the mass was hyperintensive compared to the cerebrospinal fluid (CSF) (Fig. 1B) and was rather isointensive in the T2-weighted image (Fig. 1A). The mass was enhanced mildly, not densely (Fig. 1C).

Preoperative magnetic resonance images (MRI): Intradural extramedullary mass of 1.8×1.6×4 cm size was found on the L4-5 in a MRI. The mass was isointensive in the T2-weighted image (A) and mild hyperintensive in the T1-weighted imange (B) and enhanced mildly (C).
A total L5 laminectomy and L4 partial laminectomy with gross total tumor removal were carried out (Fig. 2). The tumor mass was gray-colored and so fragile that it was easily removed (Fig. 3). However, the tumor capsule was so adhered to neural tissue there was some difficulty dissecting it. Histopathological examination demonstrated a squamous-lined cyst with keratin debris, and histological diagnosis confirmed a epidermoid cyst without malignancy (Fig. 4). After the operation, the patient showed remarkable neurological recovery.
Postoperative magnetic resonance imaging: The mass was gloss total removed.
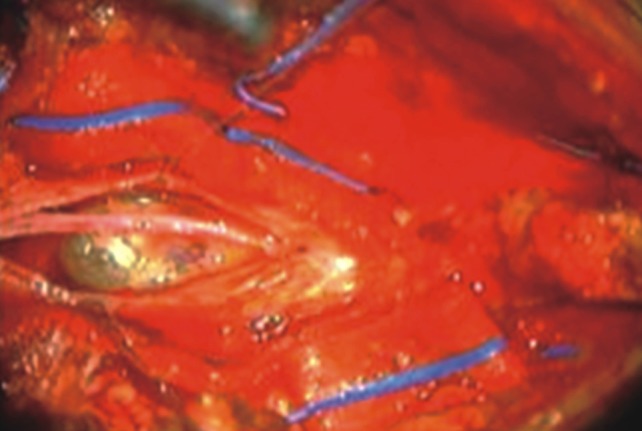
Intraoperative photography: A capsulated gray colored mass was found.
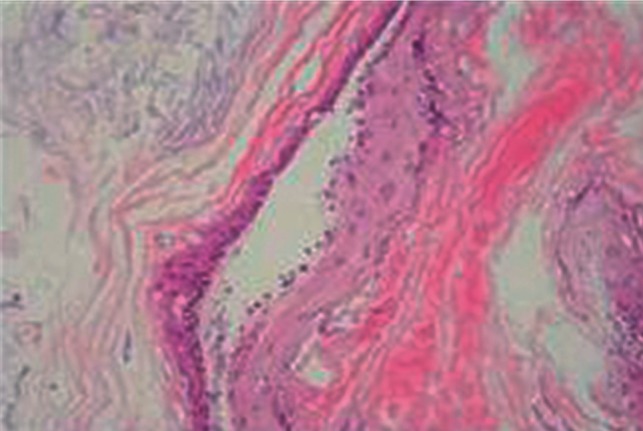
Microscopic findings: On photomicrograph of histologic specimen, desquamated cells containing keratohyalin encased within a laminated capsule of well-differentiated stratified squamous epithelium. Histologic diagnosis confirmed epidermoid cyst without malignancy (H&E, ×100).
DISCUSSION
Epidermoid tumors are represented histologically by a mass of desquamated cells containing keratohyalin encased within a laminated capsule of well-differentiated stratified squamous epithelium. Pathogenetically, these tumors may be secondary to congenital development or iatrogenic implantation. Congenital tumors are associated with spinal malformations, such as spina bifida and other dysraphic states, with a greater tendency to develop in thoracic spines11).
Many cases of epidermoid cyst development have since been described in patients with a history of lumbar puncture, and Korea is no exception3,6,7,8,10). In 1962, Manno9) reported 41% of patients with spinal epidermoid cyst had a history of lumbar puncture. Gibson and Norris4) mentioned that skin fragments had been left in needles in 70% of cases when skin puncture had been done without a stylet. According to the Van Gilder and Schwartz5) study in rats, intraspinal epidermoid tumors after skin implantation had occurred in 89% of young rats. Through this study, it became widely known that epidermoid cysts can be acquired when using needles without a stylet or with an ill-fitting stylet for lumbar puncture because parts of epithelial layers could be infilterated to spinal cavities.
The most frequent site of congenital spinal epidermoid tumor is the intramedullary thoracic segment, while the tumors acquired during lumbar puncture are generally located posteriorly in the lumbar inter space and intradural extramedullary space of the conus medullaris the cauda equina segment.
MRI can show a typical homogeneous or heterogeneous hypointense signal on T1-weighted image and hyperintense signal on T2-weighted image1). However, epidermoid tumors showing atypical signal intensity changes have been reported, such as hyperintense signal on T1-weighted image and hypointense signal on T2-weighted image, as seen in our case. This variability in signal characteristics, which might be related to the chemical state of cholesterol or the relative composition of cholesterol and keratin, makes preoperative diagnosis difficult1). Additionally, no contrast enhancement is seen in most cases, but enhancement of a thin peripheral rim has been reported13).
Our patient had no other congenital malformations and had a history of 3 times lumbar punctures for pneumococcal meningitis. Although she had no imaging before, such as myelography or MRI, a pre-existing tumor could be excluded. Lumbar puncture levels were also not reported, so their locations could not be verified. However, it can be suggested that this spinal epidermoid cyst had developed as a complication after lumbar puncture because no other anomalies had been found in the patient's 21 years, symptoms had occurred in the 8 years after lumbar puncture, and the cyst's location at L4-5 level corresponded with a frequent puncture site. Time between puncture and onset of symptoms was 2-23 years in one study9).
There is a possibility that use of a hollow needle without stylet, an ill-fitting stylet, and young age may be associated with development of the epidermoid cyst.
CONCLUSION
The present case emphasizes the fact that epidermoid tumors can occur after lumbar puncture. Patient without congenital defects of the spinal column but with history of lumbar puncture should be aware of potential adverse complications, such as epidermoid tumors, although their incidence may be low. In cases of intradural tumors or tumor-like lesions showing high signal on T1-weighted image without central enhancement, spinal epidermoid cysts should be considered.