Cervicogenic Vertigo Treated by C1 Transverse Foramen Decompression : A Case Report
Article information
Abstract
Cervicogenic vertigo was known as Bow hunter's syndrome. Occlusion of vertebral artery causes vertebrobasilar insufficiency and we reported cervicogenic vertigo case which was treated by simple decompression of transverse foramen of C1. The patient was 48 years old female who had left side dominant vertebral artery and vertigo was provoked when she rotated her head to right side. Angiography showed complete obliteration of blood flow of left vertebral artery when her head was rotated to right side. The operation was decompression of left vertebral artery at C1 level. Posterior wall of transverse foramen was resected and vertebral artery was exposed and decompressed. After surgery, vertigo of the patient was disappeared, and angiography showed patent left vertebral artery when her head was rotated to right side. Vertigo caused by compression of cervical vertebral artery could be treated by decompression without fusion or instrumentation, especially in C1 transverse foramen.
INTRODUCTION
Vertigo is a common symptom that physicians may meet in their clinical activities. Vertigo is sometimes associated with intracranial lesion or ontological lesion. Rarely, vertigo may be caused by cervical spine lesion which is known as Bow hunter's syndrome1). Bow hunter's syndrome is symptomatic vertebrobasilar insufficiency (VBI) caused by occlusion of the vertebral artery in cervical spine which is provoked by head rotation2,6,11,12). Typical symptoms include diplopia, dysarthria, visual disturbances, nystagmus, vertigo and ataxia5,7). Several reports suggested various treatment methods such as conservative management, surgical decompression of vertebral artery and endovascular treatment2). We report a patient with classical bow hunter's syndrome who was treated by decompression of C1 transverse foramen.
CASE REPORT
A 48 years old female visited with repeated vertigo attack which had emerged when she rotated her head to right side. She also complained of tinnitus on left side simultaneously. She had otitis media at left ear in the past but treated well and vestibular test showed normal result. On physical examination there was no neurologic deficit in neutral position, but left side nystagmus was found when her head was rotated. Computed tomographic angiography (CTA) showed that left vertebral artery was dominant and right vertebral artery was hypoplastic (Fig. 1). Angiography was performed in supine position. Arterial filling and patency was intact in neutral position. But in right side head rotation position, the patient experienced vertigo attack and angiography showed occlusion of left vertebral artery (Fig. 2). Surgical decompression was performed. After induction of general anesthesia, the patient was positioned in prone position and her head was mildly flexed. Midline vertical was incised and C1 posterior arch & C2 spinous process was exposed. A part of left posterior arch and transverse foramen of C1 were removed by kerrison rounguer and high speed drill (Fig. 3). Posterior side of vertebral artery was exposed and its pulsatile movement was observed after decompression. Gelfoam was applied on the decompressed site and wound was closed layer by layer. Immediately after surgery, the patient's symptoms were decreased. Vertebral artery angiography was performed 1 month later and occlusion of left vertebral artery during right side head rotation was not observed anymore (Fig. 4). The patient did not have vertigo attack again.
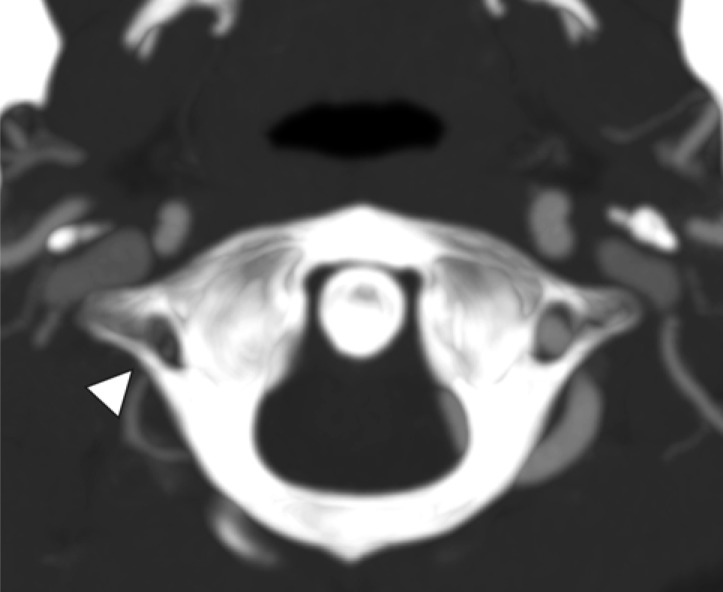
Preoperative computed tomographic angiography at C1 vertebra level in axial view. Right vertebral artery was hypoplastic than left side one (Arrowhead).
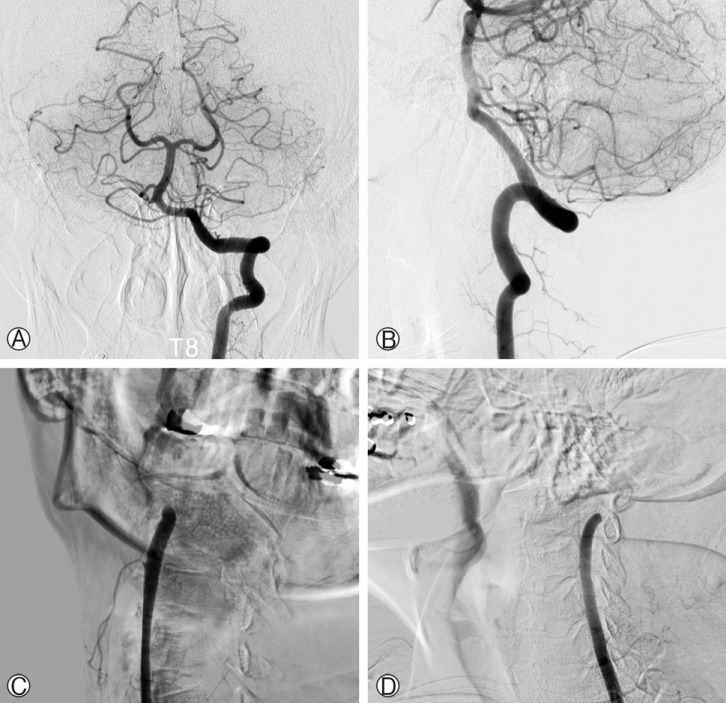
Cerebral angiography in neutral position and rotation of head to right position. Patency of left vertebral artery flow was seen in AP view (A) and lateral view (B). When the patient's head was rotated to the right side, flow of vertebral artery was obstructed at C1 transverse foramen level in AP view(C) and lateral view (D).
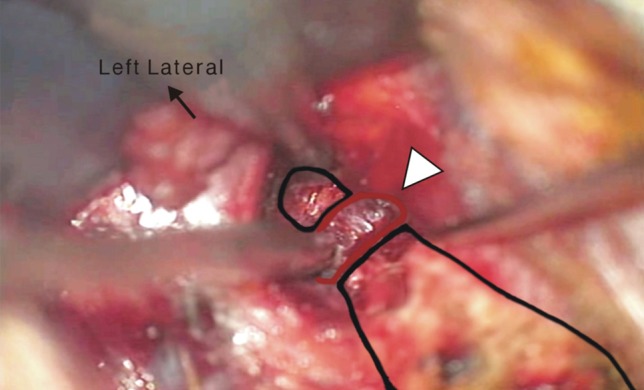
Intraoperative microscopic view. Removal of posterior bony structure of C1 left transverse foramen. Black line indicate left side of posterior arch of C1 and red line indicated left vertebral artery. Vertebral artery was decompressed well (Arrow head).
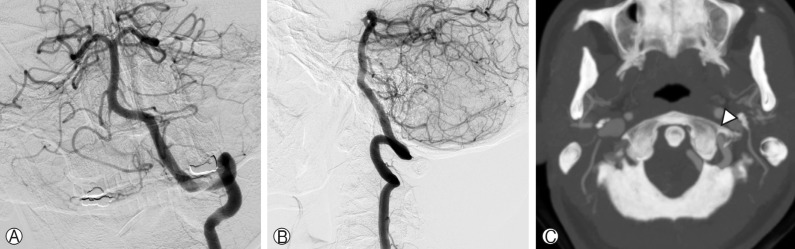
Postoperative angiography and CT angiography. Blood flow was maintained in head rotation position (A and B). Posterior wall of left transverse foramen was resected (Arrow head) (C).
DISCUSSION
Dizziness and vertigo is frequently met in clinical activities of neurosurgeons and there are many causes. In rare cases, these symptoms may be caused by vertebral artery occlusion at cervical spine and causes VBI. Numerous causes of VBI are reported of which the most common cause is arthrosclerosis of the arteries distributed in the brain stem1). Osteophytes, cervical musculature, fascial bands, anomalies of cervical spine and vertebral artery are other extracranial mechanical causes of VBI1,9). Most of reported cases in bow hunter's syndrome showed occlusion of a dominant vertebral artery due to mechanical stretching or compression and dislodgment between C1-2 with head rotation8). Our case did not show above features but occlusion of vertebral artery was limited in transverse foramen of atlas. This bow hunter's syndrome was difficult to diagnose without suspicion of cervical spine lesion of vertebral artery2,4,9).
Gold standard for diagnosis of bow hunter's syndrome is conventional angiography in various motion of cervical spine2). This case showed complete occlusion of blood flow of left vertebral artery when the head was rotated to right side. Computed tomography angiography is needed to understand structural correlation between vertebral artery and bony component of cervical spine. Magnetic resonance image also may be helpful for identifying ischemic change of cerebellar parenchyma or stability of cervical spine. Transcranial Doppler examination may be needed to check blood flow of vertebral artery without radiation exposure.
Mechanical decompression of vertebral artery is the most favorable treatment goal for bow hunter's syndrome. In mild cases, conservative treatment such as cervical brace appliance, limitation of neck motion and anticoagulation medication is helpful for symptom relief. Surgical decompression may be considered when these conservative methods fail. Numerous literatures report decompression of vertebral artery with or without fusion surgery achieved favorable outcome6,8,10,13). But there was limitation of neck motion after fusion surgery, especially in C1-2 fusion. Takeshi reported total relief of vertigo in fusion surgery patients but only 66.7% relief of symptoms in decompression surgery patients8). This may be due to complex structure of C1-2 lesion. Surgical methods should be determined after careful evaluation. Other treatment option is endovascular surgery. Darkhabani et al reported 4 cases of bow hunter's syndrome and vertebral artery stenting at V2 segment (C2-C6 level) had been achieved complete relief of their symptoms3). Our case was treated with decompression only of left side transverse foramen of C1 where mechanical compression had occurred, and the patient was relieved from symptoms without limitation of cervical spine mobility. If compromise of vertebral artery is limited in bony structure of transverse foramen, direct decompression without fusion or screw fixation may be the best option for preserving cervical spine motion.
CONCLUSION
Vertigo caused by head rotation may be suspected as vertebral artery insufficiency such as bow hunter's syndrome. Angiography is essential for diagnosis and decision of surgical treatment and adequate decompression of dominant vertebral artery without fusion surgery could achieve favorable outcome.