Anterior Screw Fixation of Anteriorly Displaced Type III Odontoid Fracture Corrected by Transoral Digital Manipulation
Article information
Abstract
Type III odontoid fractures have been treated by several methods. In case of anteriorly displaced type III odontoid fracture which is not corrected by closed reduction, anterior screw fixation cannot be used. We report the first case of anterior screw fixation of anteriorly displaced type III odontoid fracture corrected by transoral digital manipulation.
INTRODUCTION
The type III odontoid fracture is the second most common fracture among odontoid fractures1,5). It was accepted that the type III odontoid fracture was usually healed by nonoperative treatment. As a surgical method, anterior screw fixation provides a high fusion rate and preservation of cervical rotation. If there was displacement of fracture which was not corrected to acceptable alignment, anterior screw fixation could not be performed. In a review of literatures, there are two reports about transoral intraoperative reduction of displaced dens in type II odontoid fracture4,9). We report the first case of anterior screw fixation of anteriorly displaced type III odontoid fracture corrected by transoral digital manipulation.
CASE REPORT
A 30-year-old man was transferred to the emergency department due to neck pain by falling down. There was no neurological deficit on admission. Cervical computed tomography (CT) showed the type III odontoid fracture accompanying partial fracture of left superior articular process of the axis (Fig. 1A) and a 5.4-mm anterior displacement of the dens (Fig. 1B). Cervical magnetic resonance imaging showed an intact transverse atlantal ligament and no spinal cord injury. Gardner-Well tongs skull traction was performed. A reduction of displaced dens was failed. We decided to perform a surgery for intraoperative reduction and stabilization. Under general anesthesia with somatosensory evoked potential and motor evoked potential monitoring, closed reduction using distraction with flexion and extension was failed. A surgical assistant attempted to compress the posterior oropharynx via the patient's mouth under simultaneous fluoroscopic visualization. A fluoroscopic image showed a reduction of displaced bone fragment (Fig. 2B). Anterior lag screw fixation was achieved under continuous transoral digital compression, but complete reduction was not achieved (Fig. 2C). There was no neurological abnormality intraoperatively and postoperatively. After six months, he did not complain neck pain and show a limitation of cervical rotation. Radiographs showed an osseous union, although that the posterior margins of both dens and axis body were not matched after six months (Fig. 3A). There was no instability in dynamic flexion-extension X-rays (Fig. 3B, C). After one year, the patient was lost to follow-up.

Cervical CT shows the type III odontoid fracture accompanying partial fracture of left superior articular process of the axis A and a 5.4-mm anterior displacement of the dens B.
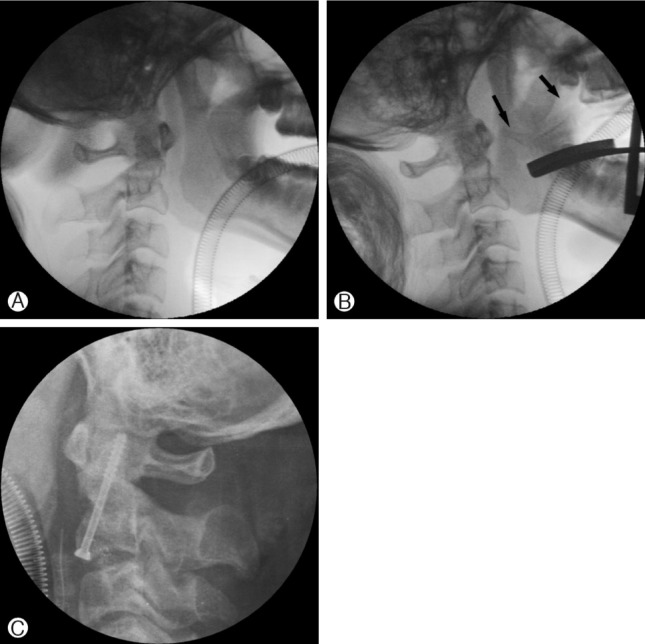
Intraoperative images shows anterior displacement of the dens A: reduction by transoral digital compression (arrow; finger) B. The anterior odontoid lag screw fixation was achieved C.

Radiograph after 6 months shows an osseous union with anteriorly displaced dens A. Flexion-extension radiographs show no instability B, C.
DISCUSSION
Anterior odontoid screw fixation is considered as a good treatment for type II and some type III odontoid fractures. It provides an immediate stabilization and preservation of cervical rotation. However, there are some contraindications. The rupture of the transverse atlantal ligament and significant comminutions of the axis body are absolute contraindication2). Relative contraindications include osteopenia, anterior or posterior obliquely sloping fractures, a fracture older than 6 months, and poor body habitus which may disturb instrument angling2,10). In the review of literatures, there are rare complications related to the instrumentation of anterior odontoid screw fixation3,8,11). These include the screw malposition, screw pullout, and screw fracture. Rarely, there is a report about delayed pharyngeal extrusion of anterior odontoid screw8).
There are many debates for treatment of type III odontoid fracture. Many authors described that it usually healed with nonoperative treatment. However, Clark and White reported a nonunion rate (10%) and malunion rate (40%) in use of a cervical collar3). Halo-device immobilization had a good result for treatment of type III odontoid fracture. Greence et al.5) reported a 1.4% nonunion rate for type III fracture in 69 cases. Julien et al.6) reported 84% bony union rate of type III fracture with a halo vest or Minerva jacket in review of literatures. As a result, the external immobilization may be chosen as initial treatment for type III fracture and surgical treatment is performed when union failed. On the other hand, Pryputniewicz et al8) mentioned that early internal stabilization might be considered if displacement was larger than 5 mm in type III odontoid fracture.
In a review of literatures, there are one case with conservative treatment and two cases with anterior odontoid lag screw fixation using transoral reduction of anteriorly displaced dens. Huber et al7) reported 3-year-old girl with odontoid synchondrosis fracture. After failure of closed reduction, they performed transoral digitally manipulated reduction followed by treatment of a Minerva plaster cast. As mentioned above, there are two reports about transoral intraoperative reduction of displaced dens in type II odontoid fracture4,8). They also used a finger compression for reduction of anteriorly displaced dens. They showed a satisfactory reduction that the posterior margins of both dens and axis body was matched postoperatively.
We decided to perform anterior odontoid lag screw fixation for immediate stabilization, preservation of cervical rotation, and early rehabilitation. Although the satisfactory reduction was achieved intraoperatively, it could not be maintained postoperatively and at the last follow-up. We think that the broader fracture base, connected with partial fracture of left superior articular process, disturbed an anatomically satisfactory reduction. However, we performed the anterior odontoid lag screw fixation with the help of such a simple manipulation. If not, the posterior stabilization should be performed and limitation of cervical rotation would be developed.
Our case indicates that transoral digital reduction may be a treatment option for irreducible anteriorly displaced type III odontoid fracture. But, the satisfactory reduction was not achieved. Long term follow-up should be needed.
CONCLUSION
We report the rare case of anterior screw fixation of anteriorly displaced type III odontoid fracture corrected by transoral digital manipulation.