Anterior Reconstruction Techniques for Cervical Spine Deformity
Article information

Abstract
Cervical spine deformity is an uncommon yet severely debilitating condition marked by its heterogeneity. Anterior reconstruction techniques represent a familiar approach with a range of invasiveness and correction potential—including global or focal realignment in the sagittal and coronal planes. Meticulous preoperative planning is required to improve or prevent neurologic deterioration and obtain satisfactory global spinal harmony. The ability to perform anterior only reconstruction requires mobility of the opposite column to achieve correction, unless a combined approach is planned. Anterior cervical discectomy and fusion has limited focal correction, but when applied over multiple levels there is a cumulative effect with a correction of approximately 6° per level. Partial or complete corpectomy has the ability to correct sagittal deformity as well as decompress the spinal canal when there is anterior compression behind the vertebral body. If pathoanatomy permits, a hybrid discectomy-corpectomy construct is favored over multilevel corpectomies. The anterior cervical osteotomy with bilateral complete uncinectomy may be necessary for angular correction of fixed cervical kyphosis, and is particularly useful in the midcervical spine. A detailed understanding of the patient’s local anatomy, careful attention to positioning, and avoiding long periods of retraction time will help prevent complications and iatrogenic injury.
INTRODUCTION
Cervical spine deformity (CSD) represents an uncommon yet severely debilitating condition [1]. It is further characterized by marked heterogeneity related to the various etiologies, distinct drivers of deformity, clinical manifestations, and dynamic state being the most mobile region of the spine [2]. As such, management and treatments demonstrate significant variation amongst treating surgeons with anterior vs. posterior vs. combined approaches, grades of osteotomy, and number of levels addressed [3]. Despite classification schemes and proposed treatment algorithms, the ultimate decisions will be dependent on patient and surgeon preference [4].
Anterior approaches to the cervical spine have been promoted since introduction of the technique by Smith-Robinson and Cloward beginning in 1958. Now, it is one of the most familiar and popular procedures with spine surgeons utilizing an anterior approach for more than 80% of cervical fusions [5]. In the setting of CSD, anterior reconstruction techniques represent a range of options with potential for powerful global or focal correction in the sagittal and coronal plane. Here, we review anterior reconstruction techniques for CSD including the preoperative planning necessary, complication care and avoidance, and postoperative management.
PREOPERATIVE PLANNING
CSD surgeries are technically demanding and require significant preoperative planning based on presence of radiculopathy or myelopathy with anterior or posterior compression, driver of deformity including the apical level, rigidity or flexibility of the deformity, and patient’s local anatomy. Patterns may be appreciated by understanding the interplay of primary drivers of the cervical deformity including compensatory mechanisms, associated symptoms, and outcomes based on management. Additional considerations include the patient’s bone quality, functional status, and comorbidities.
When considering goals of surgery for CSD, the primary aim must be to treat and prevent neurologic deterioration. Thus, the magnetic resonance imaging must be evaluated for compression of the spinal cord or foraminal stenosis. If there is ventral compression present in the setting of a kyphotic deformity, then an anterior approach will typically be necessary to achieve adequate decompression. Likewise, if there is foraminal stenosis present, then a posterior-only approach will risk cervical root neuropraxia with the performance of a posterior column shortening osteotomy. Even with adequate foraminotomies, if there is loss of disc height and consequently shortened foraminal height—a foraminotomy may not help when the cranial-caudal dimensions are further encroached by compression and extension. Increased thoracic kyphosis may also result in decreased foraminal area in the lower cervical spine, and predispose the patient to increased foraminal stenosis with further neck extension [6]. This can be avoided with the use of anterior interbody devices providing adequate indirect decompression and increasing the foraminal height prior to closing of a posteriorly-based osteotomy.
The primary driver of the deformity and the level of apex figures heavily into preoperative planning within the framework of global spinal harmony [7]. The Ames Cervical Spine Deformity classification outlines types of CSD, including cervical origin, cervical-thoracic junction (CTJ) origin, thoracic origin, coronal deformity, and craniovertebral junction origin [8]. Based on spinal region involved as the origin of the deformity and the level of apex the utility of an anterior approach becomes apparent. Specifically, when the apex of the deformity is at the CTJ or thoracic spine, patients will be unlikely improve in deformity related quality of life if the apex is not treated [9]. In other words, kyphosis at the CTJ or the thoracic spine, such as due to proximal junctional kyphosis after correction of thoraco-lumbar spinal deformity, requires a posterior approach aimed at reducing the T1 tilt in order to more readily match C2–7 cervical lordosis [10,11]. In general, the osteotomy performed at the apex of maximum curvature allows for a more anatomical correction. Thus, deformities of cervical origin in the sagittal and coronal plane are well-suited for anterior reconstruction, either alone or in combination with posterior release and fixation. Compared to posterior-only surgery, correction can be achieved with a lower complication risk and decreased total number of levels fused [12]. High-grade osteotomy and extension to the distal thoracic or upper lumbar spine, which may be necessary in posterior-only surgery, is associated with worse outcomes and may potentially be avoided with anterior reconstruction techniques [13,14]. Even after anterior index procedures, revision cervical surgery can be safely performed through an anterior approach with low complication risks—assuming the case is performed by an experienced surgeon in a specialized center [15].
Assessment of the rigidity or flexibility of the deformity is also crucial. A head suspension test should be performed in the office to determine rigidity of kyphotic deformity. These patients typically require more extensive osteotomies, and in cases of rigid chin-on chest deformity require traction to aid intubation. In extreme cases, anterior exposure may not be possible and a posterior release is necessary as part of a staged back-front-back surgery. Full-length standing and dynamic x-rays are needed. Patients that demonstrate cervical malalignment on extension x-rays likely indicate a need for higher grade osteotomies [16]. Computed tomography (CT) is also standard work-up to differentiate between rigid or fixed kyphosis, and to determine if there is anterior, posterior, or complete ankylosis. History of prior surgery is a clear factor, entailing identification of fusion vs. pseudarthrosis. The ability to perform either a single anterior or posterior-only approach requires mobility of the opposite column to achieve correction. If both columns appear ankylosed, a 540˚ procedure may be necessary—typically in the sequence of back-front-back. Unless, anterior overpowering of fused facets appears feasible, as part of an anteriorposterior sequence, depending on the extent and quality of the posterior fusion mass [17].
Further considerations include the patient’s local anatomy. This refers to identification of the course of the vertebral arteries, especially if planning for a corpectomy or complete uncinate joint resection. It also refers to evaluating for the presence of degenerative changes at other levels, particularly the proximal/distal end vertebrae when selecting levels for fusion. Concomitant coronal deformity must be accounted in order to be corrected with asymmetric resection of bone mass. Additionally, areas of prior fusion can be resected with a high-speed burr at the level of the disc space for anterior release if necessary.
Finally, the patient’s bone quality, functional status, and medical condition must be factored in with the surgical treatment plan. If there is osteoporosis or osteopenia present, a circumferential fusion and a longer construct with more points of fixation are favored. The patient’s functional status has implications for alignment goals, including planned undercorrection allowing the patient to look down when walking or cooking [18]. The patient’s general medical condition and comorbidities must of course be weighed. Preoperative examination also requires evaluation for dysphagia, which is prevalent at baseline in patients with CSD [19]. Examination by an otolaryngologist for recurrent laryngeal nerve dysfunction is recommended if there was prior anterior cervical surgery, which implicates an ipsilateral approach to prevent catastrophic bilateral vocal cord paralysis.
ANTERIOR RECONSTRUCTION TECHNIQUES
Ames et al. [20] described a cervical osteotomy classification system categorizing cervical osteotomies from grades 1–7 that increase in extent of soft tissue and bony resection, destabilization and correction potential. These osteotomies also vary in surgical approach. This article will focus on osteotomies that are performed through an anterior surgical approach. As such, all of these techniques require a mobile posterior column as determined by preoperative dynamic x-rays and CT, or by performing a posterior release as a staged approach.
All techniques generally require the same approach. As mentioned, the side of surgery will depend on previous anteriorly based surgery, and presence of any vocal cord dysfunction on preoperative examination. If there is none, the senior author (SKC) prefers to approach from the left side due the anatomically more distal location of the recurrent laryngeal nerve and theoretically lower risk of iatrogenic injury [21]. The surgical incision is planned horizontally and is placed along any prominent skin-folds present. The length of the incision is increased to correspond with the number of levels of surgery, which is possible even in the case of C2–T1 anterior fusion after sufficient soft tissue dissection. The standard Smith-Robinson approach is carried out, and the omohyoid is divided in almost all cases of multilevel surgery as it acts as a tether on the esophagus during retraction.
After accessing the anterior cervical spine, care is taken to gently release the longus colli muscle attachments using a combination of bipolar cautery and Penfield #1 subperiosteal dissection. These muscles serve an important stabilizing function, analogous to the multifidus of the lumbar spine, and form a sleeve along with the dorsal neck muscles to provide postural control [22]. The use of the Penfield #1 also allows for safe dissection laterally to fully expose the uncovertebral joints without risk to the vertebral artery (Fig. 1). Bleeding encountered with this technique is easily controlled with cautery or a hemostatic paste mixed with thrombin solution and placed under pressure with a cottonoid. Removal of large anterior osteophytes, either with a Leksell rongeur or high-speed burr, may be required prior to placement of self-retaining retractors. Narrow blades with small teeth are preferred and provide sufficient visualization of a single-disc space at a time. Anterior approaches involve removal of posterior osteophytes and resection of the posterior longitudinal ligament (PLL) allowing for complete anterior release.
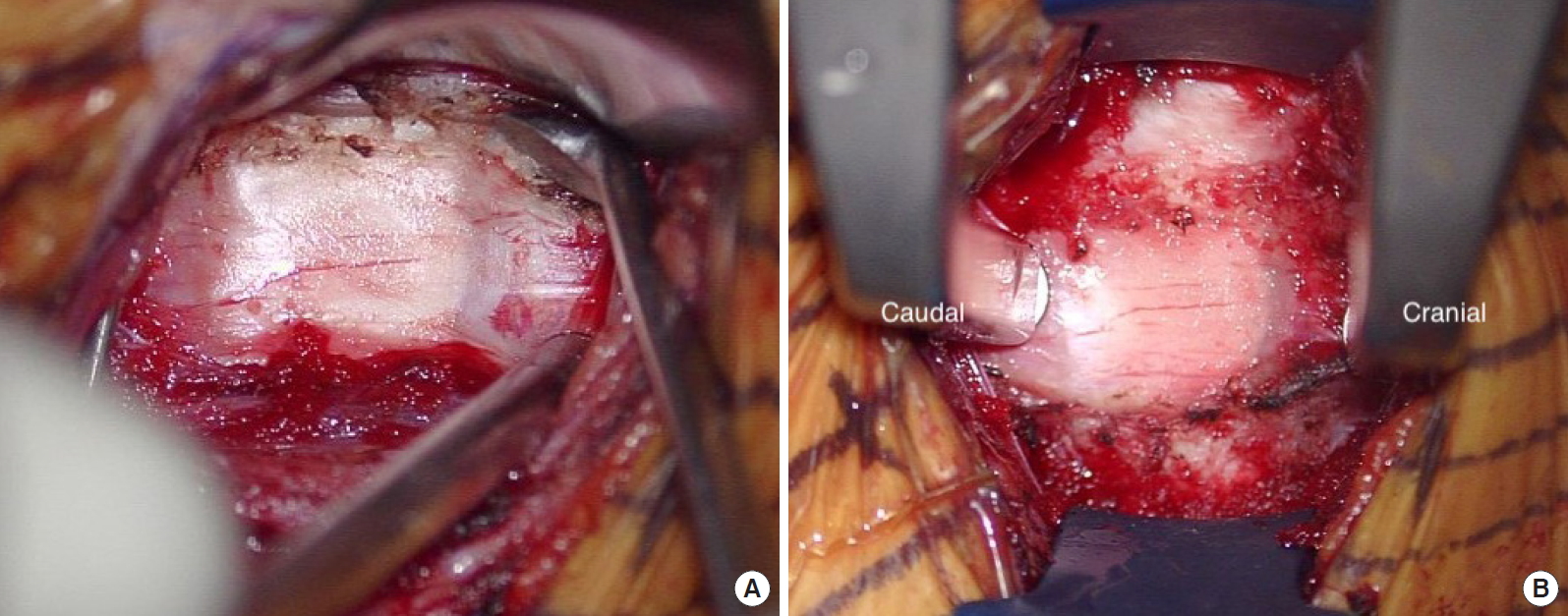
Uncinate to uncinate exposure. Intraoperative photo. (A) The longus collis can be dissected out to the lateral aspect of the uncinate by peeling it off the bone with the sharp “spoon” end of Penfield #1 in an atraumatic manner. (B) Final exposure with narrow-toothed blades and Caspar pin distraction. Final exposure should be from one uncinate to the other uncinate to perform complete anterior release.
1. Anterior Cervical Discectomy and Fusion
Grade 1 osteotomies are those of partial joint resection and can be performed through anterior or posterior approaches. The anterior approach begins with a discectomy followed by a partial resection of the uncovertebral joint. Thus, careful attention must be made to the uncovertebral joints on preoperative CT to determine if partial resection will be an adequate release. When performed in isolation across 1 or 2 levels, this low-grade osteotomy has limited local correction of 6.45° at 1 year [23]. However, when applied over multiple levels there is a cumulative effect on realignment, with a mean global correction of 32.0° if 5 levels are addressed – or again approximately 6.4° per level [24]. Segmental lordosis may be obtained through several techniques. If the bone quality is sufficient, then use of Caspar pins placed convergently will create lordosis when distraction is applied. However, if there is significant osteopenia this may cause screw plowing and loss of fixation for subsequent anterior plating and instrumentation. This may be avoided with the use of intervertebral body spreaders along with sequentially taller spacers for controlled dilation of the disc space [24,25]. Thus, multilevel anterior cervical discectomy and fusion can be an effective tool in restoring cervical lordosis.
However, there is an increased risk of nonunion with multilevel constructs and supplemental posterior arthrodesis may be added improve the fusion rate [26]. Posterior fusion may only be for additional stabilization, in which case no posterior osteotomies are performed, or along with partial or complete facet resections for further sagittal plane correction. If circumferential fusion is planned, one may make use of zero-profile interbody devices that otherwise would not be considered for a standalone multilevel construct (Fig. 2) [27,28]. Alternatively, interbody cages with integrated screws with additional anterior plate fixation provides 3 points of fixation into each segment (one screw from the cage and 2 screws from the anterior plate) and offers significant stability (Fig. 3).
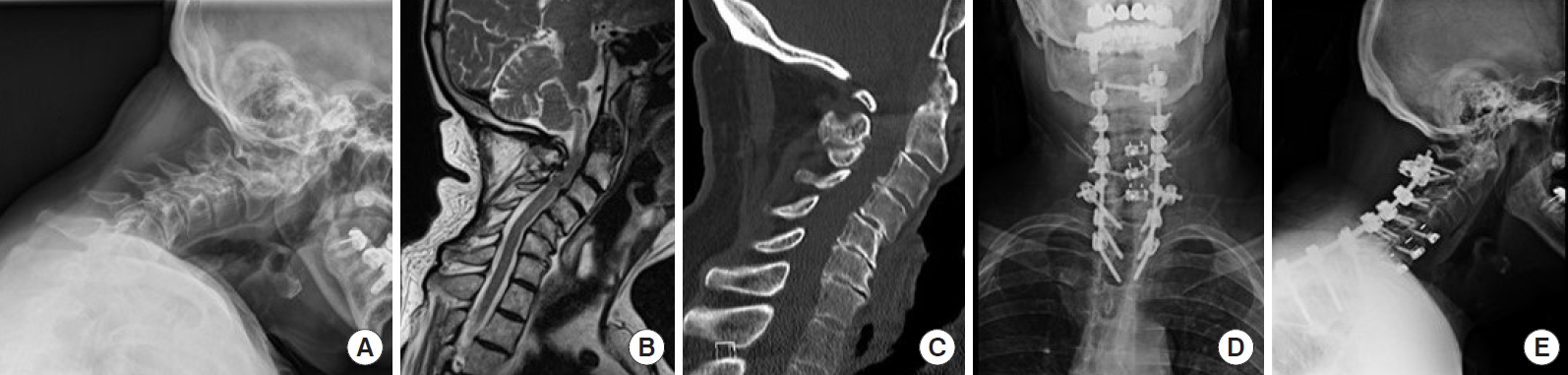
Preoperative neutral lateral x-ray (A), magnetic resonance imaging (B), computed tomography (C), and postoperative anteroposterior (D) and lateral x-rays (E) of a 79-year-old man with neck pain, dysphagia, and inability to look ahead. Underwent C4–7 ACDFs, interbody cages with screw fixation to only one vertebral body allowing each level to remain mobile and allow for further correction of kyphotic deformity with Ponte osteotomies performed from C4–7 with cantilevering and compression maneuvers posteriorly. A C2 laminar screw with an offset was placed for additional proximal fixation.

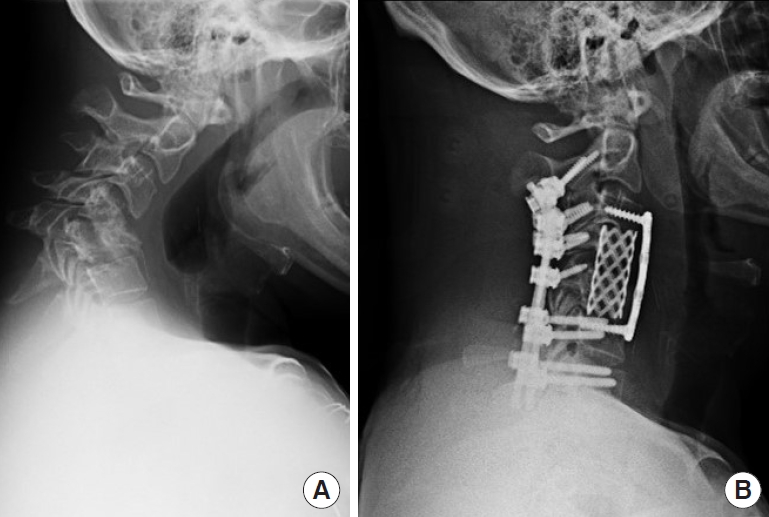
Preoperative neutral lateral x-ray (A), extension x-ray (B), magnetic resonance imaging (C), computed tomography (D), and postoperative lateral x-ray (E) demonstrating rigid midcervical kyphosis treated with C3–7 grade 1 anterior osteotomies with discectomy and placement of titanium interbody cages with integrated screws with additional anterior plate fixation to increase rigidity to obviate the need for posterior instrumentation.
2. Anterior Cervical Corpectomy and Fusion
Grade 3 osteotomies involve partial or complete corpectomy through an anterior approach. The osteotomy begins with a discectomy above and below the level of interest, followed by resection of the desired vertebral body. Partial or complete corpectomy has the ability to correct sagittal deformity as well as decompress the spinal canal and neural foramina when there is anterior compression behind the vertebral body, such as in the case of ossification of the posterior longitudinal ligament and kyphotic deformity with K-line (-) alignment [29]. This approach may also be necessary when there has been trauma or lysis from tumor or infection compromising the structural integrity of the vertebral body (Fig. 4). In a retrospective study of 145 patients with cervical spondylotic myelopathy, a grade 3 osteotomy increased cervical lordosis by 6.6° at 5-year follow-up [30]. Another long-term study by Andaluz et al. [31] found that 1- and 2-level corpectomy was effective in 130 patients with cervical myelopathy or mixed cervical myelopathy and radiculopathy. They reported an increase of 2.3° of lordosis and a 96% fusion rate in a heavy smoking population.
Preoperative neutral lateral x-ray (A) and postoperative lateral x-ray (B) of untreated trauma led to rigid kyphosis in the midcervical spine, requiring 2-level anterior cervical corpectomy and cage placement for reconstruction with supplemental posterior fixation.
In the case of 2- or 3-level corpectomy, anterior plating alone is associated with early failure and the use of adjunctive posterior fixation is recommended [32]. If feasible, a hybrid corpectomy and discectomy fusion has been shown to be superior to 2-level corpectomy with increased postoperative cervical lordosis, higher fusion rate, lower rate of subsidence, reduced risk of complications, and less blood loss [33]. The additional points of fixation at an extra segment for the anterior plate affords a more biomechanically stable reconstruction in anterior alone, long segment reconstruction procedures [34]. The addition of adjacent hyperlordotic interbody cages will also supplement correction in cases of planned circumferential fusion (Figs. 5, 6).
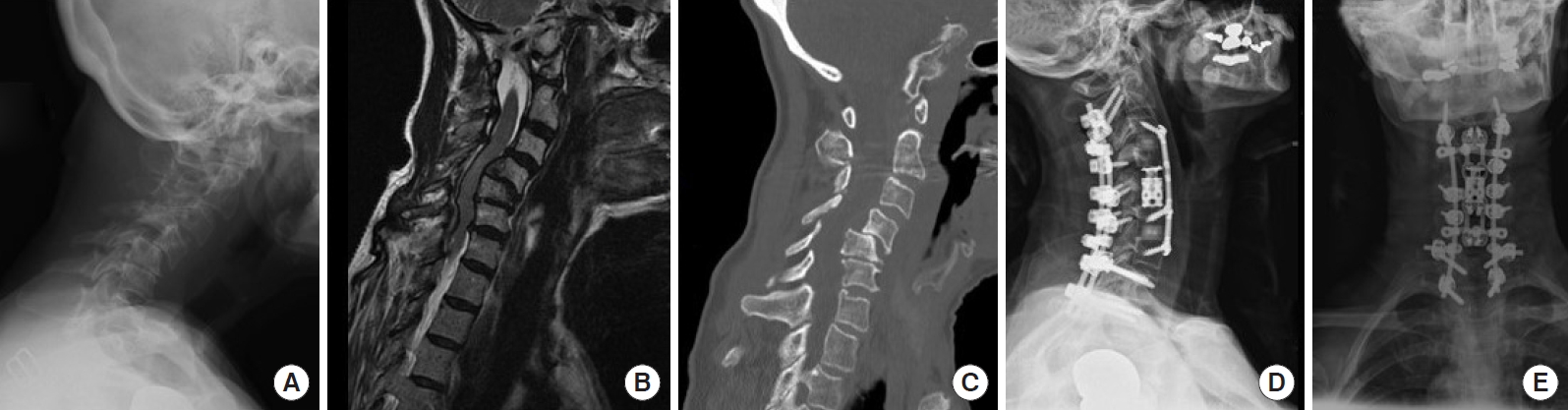
Preoperative neutral lateral x-ray (A), magnetic resonance imaging (B), computed tomography (C), and postoperative lateral (D) and anteroposterior x-rays (E) featuring a high-grade spondylolisthesis with kyphosis requiring 1-level corpectomy for decompression and 1-level supra- and infra-adjacent anterior cervical discectomy and fusions to further correct the kyphotic deformity with posterior instrumentation.
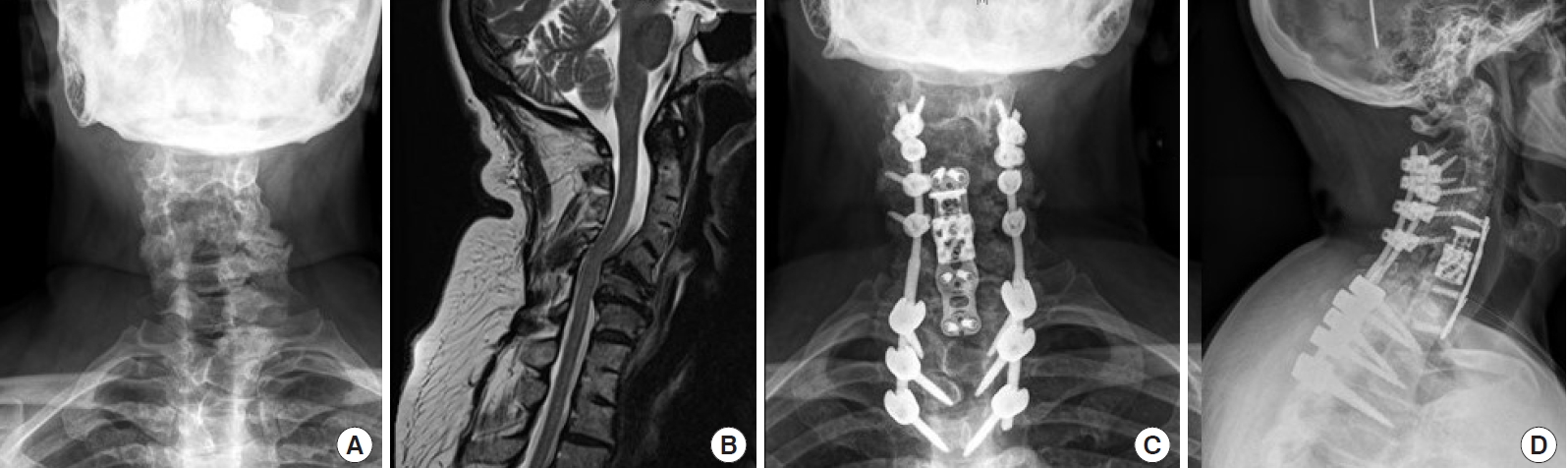
Preoperative anteroposterior (AP) x-ray (A), magnetic resonance imaging (B), and postoperative anteroposterior (C) and lateral x-rays (D) of a patient with Klippel-Feil syndrome and multiple congenitally fused cervical and thoracic vertebrae with intervening mobile segments resulting in cervical kyphoscoliosis treated with 1-level corpectomy and infra-adjacent level anterior cervical discectomy and fusion plus posterior instrumentation.
3. Anterior Cervical Osteotomy
Similar to the grade 1 osteotomy, the grade 4 osteotomy involves anterior discectomy with the addition of complete resection of the uncovertebral joint [35]. The longus colli is elevated slightly more lateral than usual, as demonstrated in Fig. 1, allowing for complete visualization of the uncinate process. After complete removal of disc material, a Penfield #4 is used to identify the lateral aspect of the uncinate process and protect the vertebral artery. Once the uncovertebral joint is clearly identified medially and laterally, an uncinectomy can be performed with the use of a high-speed burr until a thin shell of bone is left while the assistant continuously protects the vertebral artery. Care must be taken to perform the resection parallel to the disc space to prevent an iatrogenic coronal plane deformity, unless in there is coronal deformity present and a plan for asymmetric resection for realignment. The osteotomy is taken all the way posteriorly through any osteophytes to the level of the PLL. The use of an osteotome has also been described as a safe and efficient method for complete uncinectomy [36].
Indications include fixed, focal cervical kyphosis requiring more extensive anterior release. It is particularly useful for fixed kyphosis in the midcervical spine where a pedicle subtraction osteotomy would be contraindicated due to the vertebral artery —which could result in kinking of the artery and compromising cerebral blood flow [37]. This approach also aids in decompression of the nerve root when severe osteophytic foraminal stenosis is present [38]. Kim et al. reported a series of 38 patients who underwent anterior cervical osteotomy for rigid cervical deformity with a mean angular correction of 23°, and increased to 33° if combined with a posterior column osteotomy. Great caution and thorough understanding of the anatomy of the uncus, transverse foramen, and vertebral artery is required prior to performing this osteotomy [39]. Supplemental posterior fixation is advocated in all cases given the large degree of angular correction [27].
4. Complete Vertebral Column Resection
The grade 7 osteotomy is a powerful corrective tool that is only reserved for severe cases [37,40]. This osteotomy involves a complete resection of at least one vertebral body with the associated superior and inferior discs, uncovertebral joints, laminae, and facet joints. Due to the extensive bony resection require, the grade 7 osteotomy may only be performed through a combined anterior and posterior approach. This like other combined anteriorposterior procedures provides a great degree of sagittal and coronal correction, but increases the rate of neurologic injury, pseudarthrosis, revision surgery, and mortality [41]. Given their risk profile, grade 7 osteotomies are rarely performed with few reported cases, but is typically necessary when a congenital hemivertebra is present [42,43].
COMPLICATIONS
Complications related to cervical spinal deformity surgery correction is common, with reports in the literature ranging as high as 63% occurrence of at least 1 complication [44]. These may include dysphagia, cervical root neuropraxia, pseudarthosis, vertebral artery injury, dural tear, infection, and postoperative residual deformity among others [2,41]. Of these, anterior surgery is more closely associated with dysphagia while a posterior approach is more closely associated with postoperative radiculopathy, although both may occur with either approach [45].
Han et al. [41] compared complication rates between anterior surgical strategy and combined anteriorposterior approaches for correction of cervical kyphotic deformity in a meta-analysis. They found lower complication rates in the anterior surgical approach vs. combined approaches (33.7% vs. 48.9%), but a lesser degree of correction (23.0˚ vs. 30.0˚). Another study by Smith et al. [46] assessed early surgical complications (< 30 days) in 78 adults after cervical deformity surgery. They found the most common complications to be dysphagia (11.8%), deep wound infection (6.4%), new C5 motor deficit (6.4%), and respiratory failure (5.1%). Similar to Han et al. [41], they found rate of complication was related to surgical approach and lower in anterior only vs. posterior-only or combined surgical approaches (27.3% vs. 68.4% vs. 79.3%, respectively). Smith et al. [47] also reported on their all-cause mortality following surgery for CSD, with a mean 9.2% death within a 1.2-year follow-up. This may be attributed to a high level of comorbidities amongst patients, however deceased patients did experience a higher rate of major complication (63.6% vs. 22%).
Postoperative dysphagia is a common complication of anterior cervical reconstruction surgeries, yet remains poorly classified and its incidence in the literature ranges from 2.6 to 39% [48]. Animal models in sheep demonstrate local injury to the esophagus with moderate-to-severe edema between muscle fibers at the site of self-retaining retractor blades [49]. Thus, all efforts must be made to limit that direct pressure on the esophagus wall. This may be accomplished with using narrow blades and limiting retraction time. When a major degree of correction is planned, one may consider preoperative traction with a halo vest to allow for gradual correction and lengthening rather than abrupt stretching of the ventral soft tissues [50].
C5 radiculopathy and other cervical nerve root palsies are another poorly misunderstood phenomenon with controversial etiology [51]. Despite an unclear cause, there are several measures that should be taken to try to avoid this potentially debilitating injury. During positioning, avoid excessive downward traction on the shoulders with taping. In the case of fixed cervical kyphosis, delay any extension of the neck until the osteotomy is performed to avoid hyperextending the mobile segments. This can be accomplished by maintaining a stack of folded sheets below the head, and then removal by anesthesia during surgery. A pressure bag, normally used to increase the rate of intravenous infusion, used as a shoulder roll allows for precisely controlled amount of extension, including the ability to increase neck extension intraoperatively. If deciding between the use of discectomies or corpectomies, there is moderate evidence supporting a lower incidence of C5 palsy after multiple discectomies compared with corpectomy or discectomy-corpectomy hybrid approaches [52].
POSTOPERATIVE CARE
Postoperative care following anterior deformity correction includes close monitoring for aforementioned known complications in the immediate postoperative period including dysphagia, respiratory distress, and neurologic deterioration. In certain case, it may be prudent to keep the patient intubated after surgery. Following use of cervical internal fixation, immobilization in a cervical hard collar for 2–3 months has been proposed. Additionally, for patients who are unable to undergo immediate posterior fixation following anterior osteotomy when an anteriorposterior approach is preferred, temporary immobilization in a halo or rigid brace may be utilized until definitive posterior stabilization is performed.
CONCLUSION
CSD represents an uncommon yet severely debilitating condition marked by its heterogeneity. Anterior reconstruction techniques represent a familiar approach with a range of invasiveness and correction potential—including global or focal realignment in the sagittal and coronal plane. Meticulous preoperative planning is required to decompress neural elements to improve or prevent neurologic deterioration and obtain satisfactory global spinal harmony. A detailed understanding of the patient’s local anatomy, careful attention to positioning, and avoiding long periods of retraction time will help prevent complications and iatrogenic injury.
Notes
The authors have nothing to disclose.