Be Prepared: Preoperative Coronal Malalignment Often Leads to More Extensive Surgery Than Sagittal Malalignment During Adult Spinal Deformity Surgery
Article information

Abstract
Objective
To evaluate the effect of coronal alignment on: (1) surgical invasiveness and operative complexity and (2) postoperative complications.
Methods
A retrospective, cohort study of adult spinal deformity patients was conducted. Alignment groups were: (1) neutral alignment (NA): coronal vertical axis (CVA) ≤ 3 cm and sagittal vertical axis (SVA) ≤ 5 cm; (2) coronal malalignment (CM) only: CVA > 3 cm; (3) Sagittal malalignment (SM) only: SVA > 5 cm; and (4) coronal and sagittal malalignment (CCSM): CVA > 3 cm and SVA > 5 cm.
Results
Of 243 patients, alignment groups were: NA 115 (47.3%), CM 48 (19.8%), SM 38 (15.6%), and CCSM 42 (17.3%). Total instrumented levels (TILs) were highest in CM (14.5±3.7) and CCSM groups (14±4.0) (p<0.001). More 3-column osteotomies (3COs) were performed in SM (21.1%) and CCSM (28.9%) groups than CM (10.4%) (p=0.003). CM patients had more levels instrumented (p=0.029), posterior column osteotomies (PCOs) (p<0.001), and TLIFs (p=0.002) than SM patients. CCSM patients had more TLIFs (p=0.012) and higher estimated blood loss (EBL) (p=0.003) than SM patients. CVA displayed a stronger relationship with TIL (p=0.002), EBL (p<0.001), and operative time (p<0.001) than SVA, which had only one significant association with EBL (p=0.010). Both SM/CCSM patients had higher readmissions (p=0.003) and reoperations (p<0.001) than CM patients.
Conclusion
Amount of preoperative CM was a better predictor of surgical invasiveness than the amount of SM, despite 3COs more commonly performed in SM patients. CM patients had more instrumented levels, PCOs, and TLIFs than SM patients.
INTRODUCTION
Adult spinal deformity (ASD) affects 15%–20% of the adult population, with higher rates seen in older age groups [1]. Given the pain, disability, and decreased quality of life associated with ASD, and surgery rates have increased [2]. Despite the benefits of operative management, spinal reconstruction surgeries are long and complex operations, require significant recovery, and are associated with high rates of complications [3-5]. Correction of coronal and/or sagittal malalignment represents a formidable challenge to any deformity surgeon.
The technical objective of ASD surgery is to correct spinal alignment, and the operative plan depends heavily on the amount of coronal malalignment (CM) and/or sagittal malalignment (SM) present. Postoperative sagittal alignment targets are well-defined, with sagittal vertical axis (SVA)< 5 cm and pelvic incidence to lumbar lordosis within 10° [6]. However, coronal alignment goals are not fully understood, as previous thresholds to define CM range from a coronal vertical axis (CVA) of 2 cm [7,8], 3 cm [9-11], 4 cm [3,12-14], to even 5 cm [15], though most prior studies use a threshold value of 3 cm.
Sagittal-specific correction maneuvers include 3-column osteotomies (3COs), cantilever techniques, and construct-to-construct reduction. Coronal-specific correction techniques include asymmetric interbodies, asymmetric 3-column osteotomy (3CO), and “kickstand rod” placement [16-18]. While those mentioned above sagittal and coronal correction maneuvers have been shown to correct alignment with proper patient selection, it remains unknown which techniques are associated with more operative morbidity [19]. Whether correcting CM or SM, higher complication rates are associated with more invasive osteotomies, revision surgeries, or combined anterior-posterior approaches [19-21].
Given our incomplete understanding of how CM and SM influence operative complexity and postoperative complications, we attempted to study further the role of preoperative alignment patterns in ASD surgery. In a cohort of ASD patients undergoing corrective surgery, we sought to evaluate whether preoperative alignment affected 2 principal outcomes: (1) surgical invasiveness and operative complexity, and (2) postoperative complications.
MATERIALS AND METHODS
1. Study Design
A retrospective cohort study was conducted based on prospectively collected data from a single institution, spinal deformity center consisting of 2 spine deformity surgeons (LGL and RAL). All patients undergoing spinal reconstruction 06/01/2015-12/31/19 were included. Institutional Review Board approval was obtained.
2. Patient Population
Enrollment criteria were similar to prior studies of ASD patients undergoing spinal reconstruction [14,22]. The inclusion criteria were: age> 18 years undergoing ≥ 6 level instrumented fusion with at least one of the following radiographic criteria (Cobb angle> 30°, SVA> 5 cm, CVA> 3 cm, pelvic tilt of > 25°, or thoracic kyphosis [TK]> 60°) [23]. All patients underwent a standing, full-body low dose Stereoradiograph (EOS Imaging, Paris, France) prior to surgery. Patients were excluded if they were under age 18, undergoing < 6-level instrumented fusion, or lacked a wholebody Stereoradiograph at any of the follow-up time points. Patients were followed on a pattern of 8 weeks, 6 months, 1 year, 2 years, and 5 years.
Operatively, all but 2 patients underwent a posterior-only approach, and both patients underwent oblique, prepsoas approach for lumbar interbody cage placement. Patients with significant CM extending to the midthoracic spine usually had an upper-instrumented vertebra (UIV) of T1-3, whereas patients with solely lumbar deformity that did not include SM/CM above the midthoracic spine had a UIV of T10. Occasionally, in the case of significant proximal TK, the UIV will be C7.
3. Independent Variables
Demographic and perioperative variables were collected, including age, sex, body mass index, American Society of Anesthesiology (ASA) physical status classification, self-reported diagnosis of depression, deformity diagnosis, and primary versus revision surgery. Several preoperative radiographic variables were collected to determine the preoperative alignment group. To measure global alignment, both the continuous variables of CVA and SVA in cm were obtained. The CVA was measured by subtracting the coronal C7-plumb-line (C7PL; a vertical line dropped down from the middle of the C7 vertebral body) distance, from the central sacral vertical line (a vertical line that passes through the center of the sacrum) [24]. Similarly, the SVA was the distance from the sagittal C7PL (a vertical line drawn dropped down from the middle of the C7 body) and the posterior superior aspect of the S1 vertebral body [24]. Though CVA to the left was considered negative and to the right is positive, absolute values were used given the lack of clinical difference between left or right CM. In accordance with prior literature, CM was defined at a threshold of CVA≥ 3 cm [9-11], Similarly, though SVA can be negative or positive in relation to where C7 lies compared to the superior posterior aspect of S1, absolute values were used to standardize the malalignment; however, positive and negative values were used for each regression analysis. Additional radiographic variables included: pelvic obliquity (angle of line between superior iliac crest and horizontal) and leg length discrepancy (difference in height from femoral head to tibial plafond on full-body x-rays). The previously published Qiu classification was used to assess directionality, which categorized CM into 3 groups based on a value of 3 cm as follows: type A: CVA < 3 cm; type B: CVA > 3 cm and C7PL shifted to the concave side of the curve; and type C: CVA > 3 cm and C7PL shifted to the convex side of the curve [10].
4. Alignment Groups
Preoperatively, patients were divided into the following 4 groups based on alignment:
(1) Neutral alignment (NA): CVA < 3 cm and SVA < 5 cm; neither CM nor SM.
(2) CM only: CVA≥ 3 cm and SVA< 5 cm; CM only without SM. A case example is seen in Fig. 1.
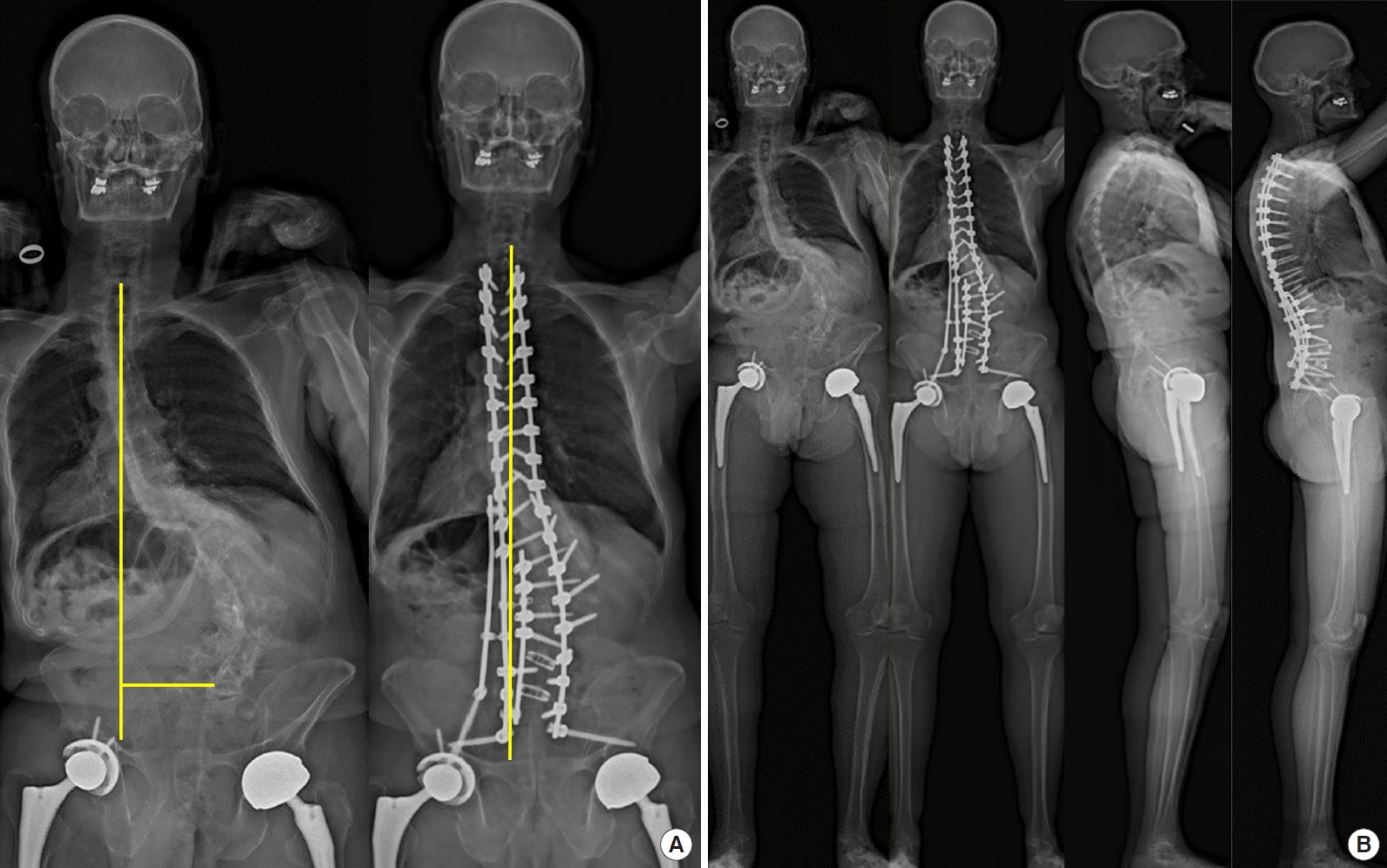
Case example of a 67-year-old male with adult degenerative scoliosis, lumbar stenosis, and 7.9 cm of preoperative coronal malalignment (CM) patient with full-spine preoperative and 2-year postoperative anteroposterior (AP) x-rays (A) and full-body preoperative and 2-year postoperative AP and lateral x-rays (B). Underwent a T2-sacrum posterior instrumented fusion, posterior column osteotomies T12–L3, TLIFs L4–5, and L5–S1, and laminectomies L3–4 and L4–5. Postoperative CM was 1.7 cm.
(3) SM only: SVA≥ 5 cm and CVA< 3 cm; SM only without CM.
(4) Combined coronal and sagittal malalignment (CCSM): both CVA≥ 3 cm and SVA≥ 5 cm, presence of both CM/SM. A case example is seen in Fig. 2.
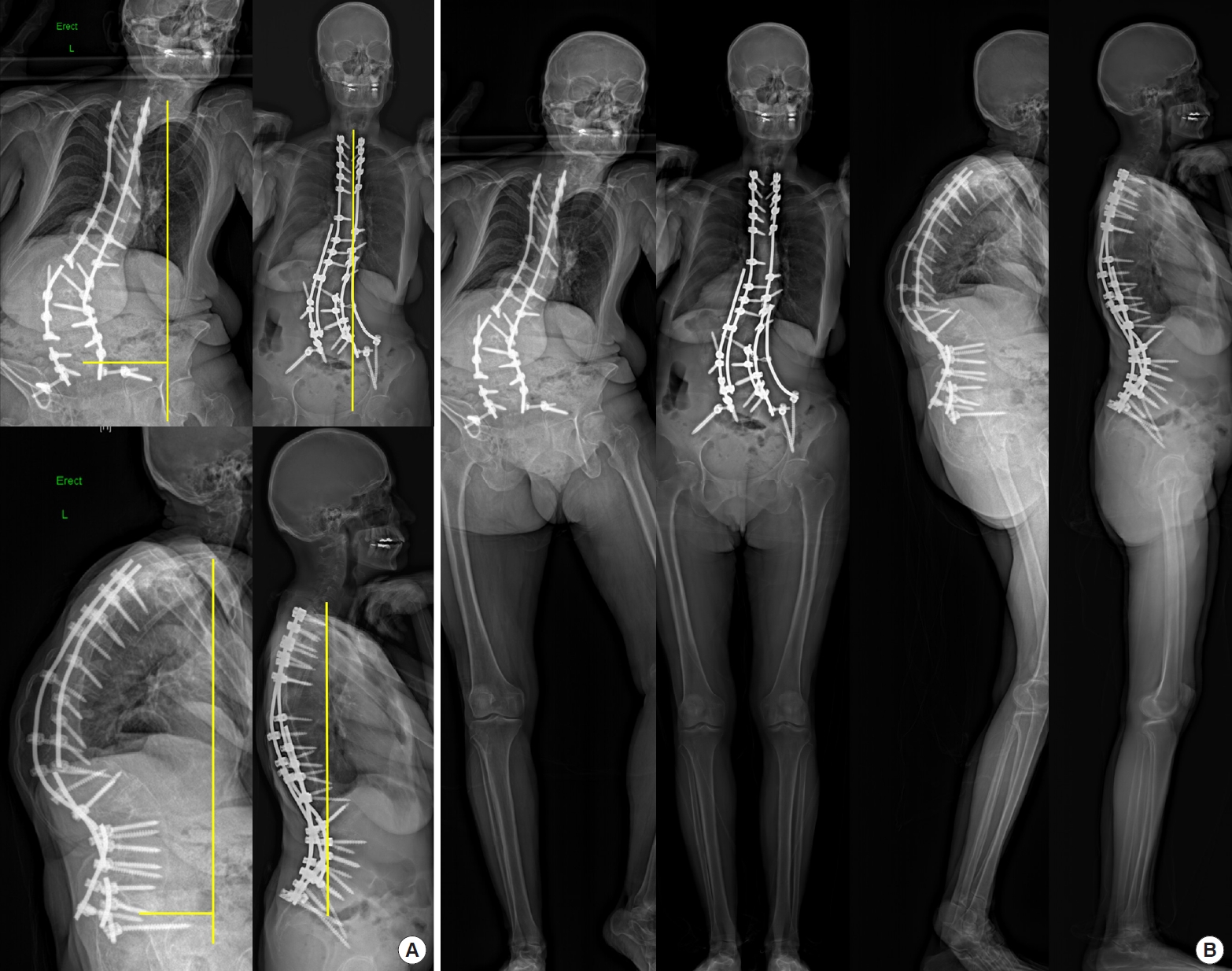
Case example of a 62-year-old female with adult idiopathic kyphoscoliosis and pseudarthrosis at L1–3, preoperative combined coronal and sagittal malalignment (CCSM) patient with full-spine preoperative and 2-year postoperative anteroposterior (AP) and lateral x-rays (A) and full-body preoperative and 2-year postoperative AP and lateral x-rays (B). Preoperative coronal malalignment (CM) was 6.62 cm and sagittal malalignment (SM) was 11.24 cm. Preoperative CM is underrepresented on x-ray as the patient is compensating on the right side by standing on the tips of her toes and bending her knee to elevate her ipsilateral hemipelvis to prevent further right-sided leaning. She had a prior T3-sacrum instrumented fusion and L2 pedicle subtracion osteotomy at an outside institution. Revision surgery consisted of instrumentation removal T3-sacrum, posterior instrumentation T1-sacrum, posterior column osteotomies T1–5/T9–L5, and placement of a right-sided kickstand rod for resolution of CCSM. Postoperative CM was 1.3 cm and SM was 0.5 cm. Postoperatively the patients’ pelvis is now level and both legs are straight demonstrating the marked improvement in alignment.
5. Primary and Secondary Outcomes
The primary outcome of interest was defined as surgical invasiveness and operative complexity. Variables involving the primary outcome included: total instrumented levels (TILs), number of posterior column osteotomies (PCOs), 3CO performed (binary), transforaminal lumbar interbody fusion (TLIF) performed (binary), unintended durotomy (binary), number of rods (continuous), presence of pelvic instrumentation (either S2-alar-iliac screws or iliac screws; binary), estimated blood loss (mL), operative time (minute), or presence of an intraoperative neuromonitoring (IOM) data loss (binary), as defined in previous studies [25]. The secondary outcome of interest was defined as postoperative complications. Variables involving the secondary outcome included: major complication according to prior literature [26], readmission, and reoperation, defined as requiring revision spine surgery. Contrary to other studies, to answer our previous research question, the variables used for outcome measures were TIL, osteotomies, and estimated blood loss to indicate surgical invasiveness.
6. Statistical Analysis
Descriptive statistics were used to summarize patient demographics and radiographic data. Categorical data were presented as frequencies and percentages, whereas continuous data were presented with mean and standard deviations. Absolute values were used for SVA and CVA to allow for statistical analysis. Based on Shapiro-Wilk tests, all variables were considered to be nonparametrically distributed, except operative time. Kruskal-Wallis tests were used to assess for differences between continuous variables, except for operative time, where a 1-way analysis of variance test was used. Chi-square proportion tests were used for count data. Univariate linear regression was used to determine an association with amount of coronal or sagittal malalignment (CVA/SVA) with the continuous variables of TIL, EBL, and operative time, followed by multivariate regression controlling for age, sex, body mass index (BMI), maximum Cobb angle, and amount of CM/SM. Statistical significance was set at an alpha level of < 0.05. All statistical analyses were performed in STATA 14 (StataCorp LP., College Station, TX, USA).
RESULTS
1. Demographics
A total of 243 patients underwent ASD surgery with a mean age was 49.3±18.3 and mean instrumented levels was 13.5±3.9. Mean preoperative CVA absolute value was 2.9±2.7 cm, and mean preoperative SVA absolute value was 5.4±5.5 cm. Overall alignment of all patients preoperatively was: NA 115 (47%), CM 48 (20%), SM 38 (16%), and CCSM 42 (17%). Demographic and preoperative variables of all patients based on alignment group are summarized in Table 1. Qiu classification preoperatively was: type A (153; 63%), type B (53; 22%), and type C (37, 15%). As expected, several between group differences were seen based on preoperative alignment.
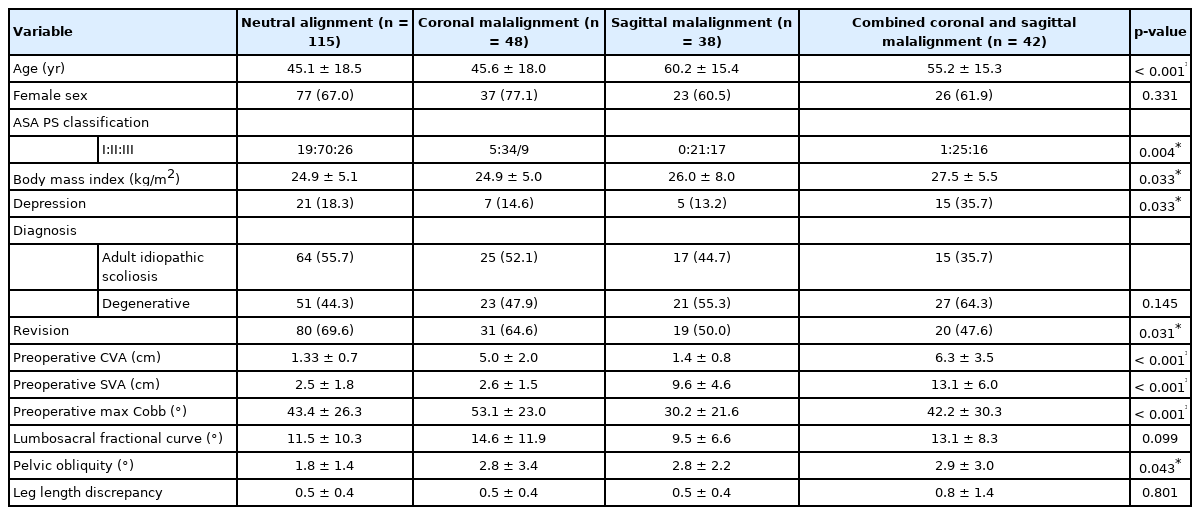
Demographics and preoperative alignment variables
2. Primary Outcome: Surgical Invasiveness and Operative Complexity
For the primary outcome of surgical invasiveness and operative complexity, significant across group differences were seen in 8 of the 10 individual variables (Table 2). The only 2 variables that did not demonstrate statistical significance across all alignment types were TIL and IOM changes. The remaining 8 variables all showed significant variability depending on alignment type, which included: PCOs (p<0.001, highest in NA and CM), 3CO (p=0.002, highest in SM/CCSM), TLIF performed (p<0.001, highest in CM and CCSM), durotomies (p=0.009, highest in CM and CCSM), number of rods (p<0.001, lowest in NA), pelvic instrumentation (p<0.001, lowest in NA), EBL (p<0.001, highest in CM and CCSM), and operative time (p<0.001, highest in CM and CCSM).
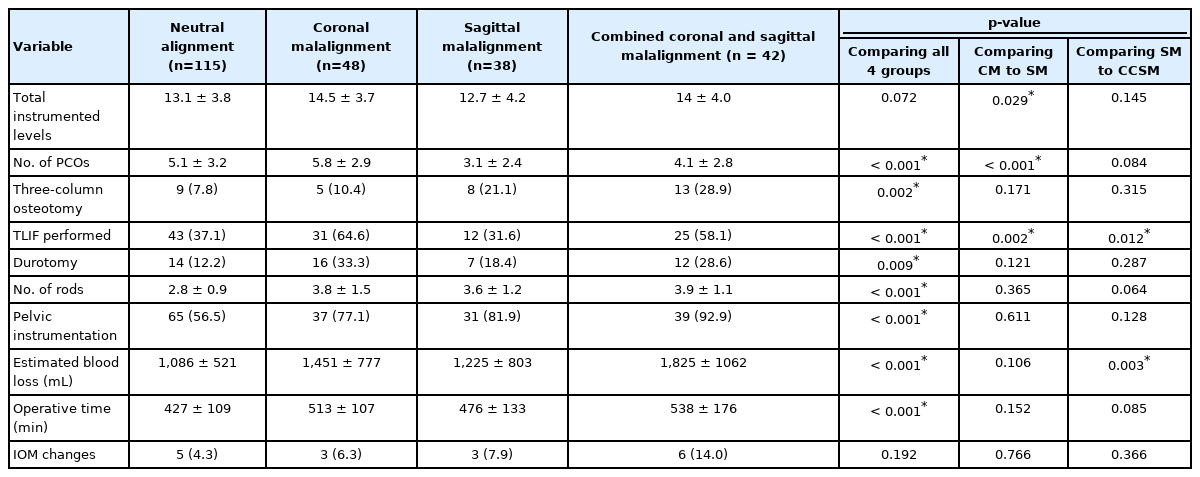
Surgical invasiveness and operative complexity based on each alignment group
Comparing CM to SM directly, groups were not significantly different except for 3 variables. The CM group had significantly more levels instrumented (14.5±3.7 vs. 12.7±4.2, p=0.029) more PCOs performed (5.8±2.9 vs. 3.1±2.4, p<0.001), and more TLIFs performed (64.6% vs. 31.6%, p=0.002) (Table 2).
Comparing SM to CCSM directly, groups were not significantly different except for 2 variables. The CCSM group had more TLIFs (58.1% vs. 31.6%, p=0.0123) and higher EBL (1,825±1,062 mL vs. 1,225±803 mL, p=0.003) (Table 2).
The relationship between amount of CM or SM and 3 individual variables of TIL, EBL, and operative time was assessed. Univariate linear regressions are depicted graphically for CVA (Fig. 3A–C) and SVA (Fig. 4A–C). After controlling for age, sex, BMI, maximum Cobb angle, and amount of CM/SM, CVA displayed a stronger statistical association with TIL, EBL, and operative time compared to SVA (Table 3). For CVA, significant relationships were seen for each variable, with a higher CVA significantly associated with increased TIL (β=0.33; 95% confidence interval [CI], 0.13–0.54; p=0.002), EBL (β=83.13; 95% CI, 46.59–119.67; p<0.001), and operative time (β=14.62; 95% CI, 8.42–20.81; p<0.001). For SVA, no significant relationship was seen between TIL (β=-0.05; 95% CI, -0.13–0.04; p=0.287) and operative time (β=2.36; 95% CI, -0.41–5.13; p=0.095), yet a significant relationship was seen between SVA and EBL (β=21.59; 95% CI, 5.24–37.94; p=0.010), where a higher SVA was associated with increased EBL.
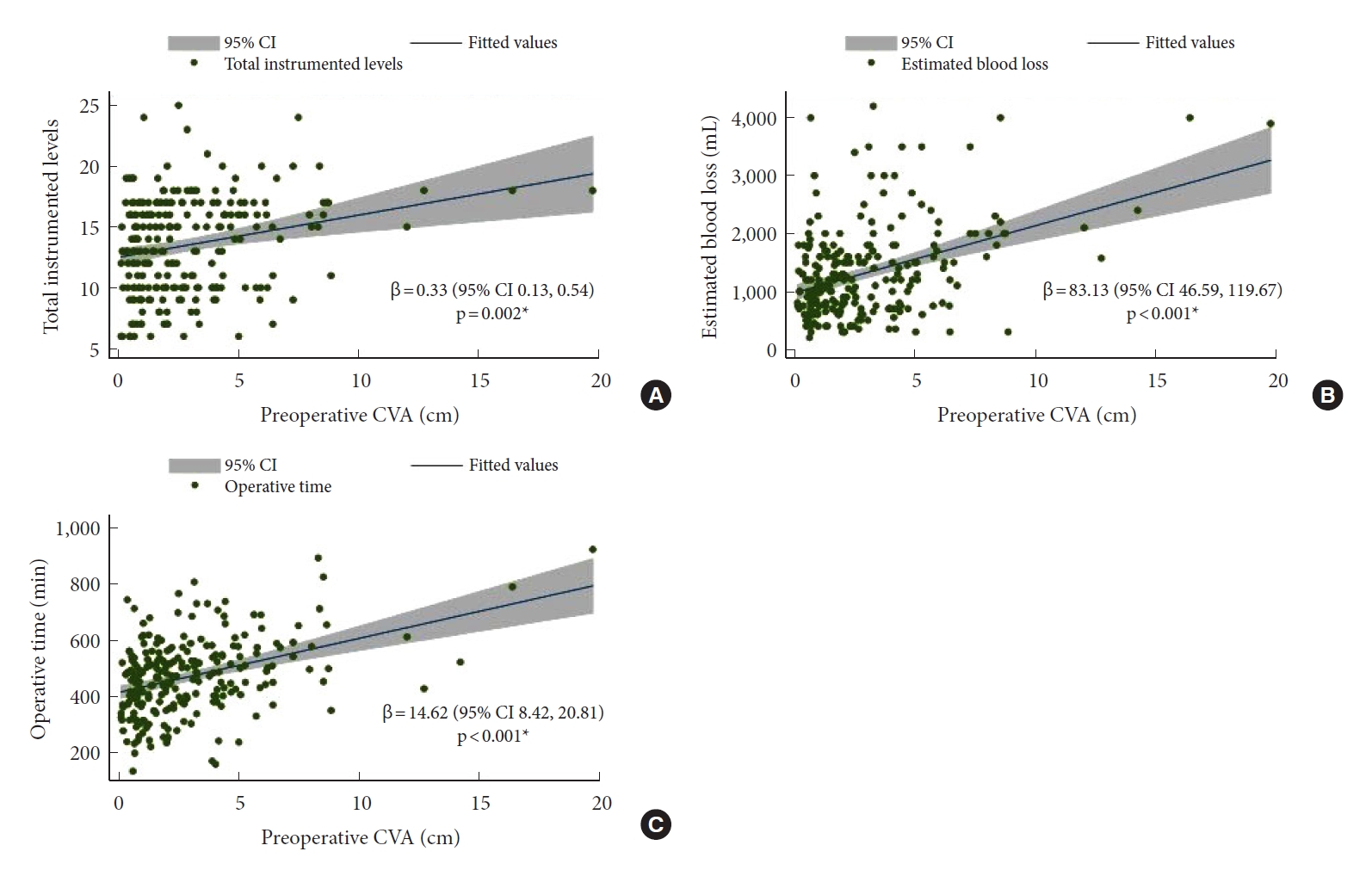
Univariate linear regressions for coronal vertical axis (CVA) with total instrumented levels (A), estimated blood loss (B), and operative time (C). CI, confidence interval.

Univariate linear regressions for sagittal vertical axis (SVA) with total instrumented levels (A), estimated blood loss (B), and operative time (C). CI, confidence interval.

Multivariate linear regression for CVA and SVA controlling for age, sex, body mass index, maximum Cobb angle, and coronal/sagittal malalignment
3. Secondary Outcome: Postoperative Complications
Follow-up at 2 years was seen in 174 patients, allowing for a 71.6% 2-year follow-up rate. Two-year alignment breakdown was: NA 82 (47.1%), CM 32 (18.4%), SM 28 (16.1%), and CCSM 32 (18.4%). For secondary outcomes, there was no difference in rates of major complications were seen across all 4 groups, yet readmission and reoperation were significantly different (Table 4). Both readmission (p=0.003) and reoperation (p<0.001) were significantly different across all 4 groups, and highest for the SM and CCSM groups.

Postoperative complications
DISCUSSION
The current study aimed to determine the effect of preoperative spinal malalignment on surgical invasiveness and operative complexity, as well as postoperative complications. We found that preoperative alignment led to a significantly different level of surgical invasiveness and operative complexity in 8 of the 10 surgical primary outcome variables. When comparing CM to SM directly, the CM group had more instrumented levels, underwent more PCOs, and had more TLIFs performed. Comparing SM to CCSM, the CCSM group had TLIFs performed more often and higher blood loss. Multivariate linear regression revealed that CVA held a statistically significant and stronger linear association with 3 operative complexity variables of instrumented levels, blood loss, and operative time compared to SVA. For the secondary outcomes of postoperative complications, SM and CCSM patients had the highest rate of readmission and reoperation. Together, these findings suggest that the amount of CM is a strong driver of the invasiveness and complexity in ASD surgery.
Perhaps the most interesting finding was that the amount of CM had a stronger association with operative invasiveness and complexity than the amount of SM. Compared to its well-studied sagittal counterpart, coronal alignment in ASD surgery has been less emphasized [18]. Whether it be due to the technical difficulties of correcting coronal plane abnormalities or lesser weight placed in operative decision-making, postoperative rates of CM remain high, ranging from 19.3% [18] to 34.8% [10] with some studies reporting higher levels of CM postoperatively than preoperatively [10,14,17,18]. One potential reason for this is that techniques to correct CM, such as adding a kickstand rod, can take additional time, leading to more blood loss and longer operative time. With respect to operative invasiveness and complexity, other studies have shown equally high rates of blood loss and operative time. Comparing 338 PSO patients to 52 asymmetric PSO patients, Lau et al. [12] reported higher EBL in the asymmetric PSO group (2,096 mL vs. 1,989 mL), though this was not statistically significant. The same trend was seen for operative time—319 minutes for asymmetric PSO compared to 307 minutes for PSO—without statistical significance. Complications were not different between both groups as well (40.3% asymmetric PSO vs. 33.1% PSO) [12]. In a cohort of patients with severe CM, Buell et al. [27] reported that patients with CVA ≥ 10 cm had an EBL of 2.5 L compared to patients SVA ≥ 10 cm with an EBL of 2.4 L. Interestingly, operative time was virtually the same for patients with SVA ≥ 10 cm (8.2 hours) compared to CVA ≥ 10 cm (8.1 hours). However, despite an informative report on severe CM, it was unknown if these patients had CCSM or CM and SM in isolation, making a comparison to the current study difficult. To our knowledge, no other reports have compared CM patients exclusively to SM patients.
Additional differences in our series showed that patients with CM and CCSM were more likely to undergo TLIFs, which likely represents the importance of horizontalizing the lumbosacral fractional curve, and creating a strong, symmetric base across the lumbosacral junction. CM patients also underwent more PCOs than 3COs, reflecting that without significant sagittal plane abnormalities, multilevel PCOs are all that is needed to correct the coronal deformity, in the absence of a rigid, fixed, sagittal deformity. Additionally, CCSM patients had longer operative time than SM patients, reinforcing the difficulty of correcting biplanar deformities. Lastly, CM patients had higher TIL than the SM group, which likely reflects that CM often occurs in the MT or TL/L segment of the spine. The cranial end of the scoliosis stops in the midthoracic area, which is a suboptimal stopping point. In comparison, SM patients may have only focal loss of lumbar lordosis that stops in the upper lumbar or distal thoracic segment, lending itself to an appropriate lower thoracic UIV.
Despite a strong association between several operative complexity variables and CVA, 3COs and reoperations were more common in patients with SM. In the setting of a prior fusion, 3COs are often required to correct fixed sagittal plane deformities and are associated with significant blood loss and high rates of complications [22,28,29]. However, despite increased frequency of 3COs in SM patients, CM still required more time to correct. Taken together, though less invasive osteotomies were performed for CM deformities, the coronal correction took more time, especially in CCSM patients. Potential reasons for this include need for a kickstand rod and difficulty placing screws in coronally malaligned patients, which is often more straightforward if only SM is seen, without lateral subluxation often encountered with significant scoliosis. Moreover, the spinal cord may not be able to tolerate extensive coronal correction over a short period, causing the surgical team to correct the coronal deformity slowly, over multiple rounds of compression and distraction. Moreover, despite longer operative time and blood loss seen with CM, SM and CCSM had the highest rate of readmissions and reoperations, highlighting the increased risk with sagittal and biplanar corrections. Others have reported similar findings, with greater preoperative SVA being a predictor of revision surgery [30]. The high rate of revision surgery among SM patients may be due to the ensuing risk of pseudarthrosis, rod fractures, and other mechanical complications seen with 3COs compared to PCOs [31].
The current study provides a deeper understanding of how preoperative spinal alignment affects surgical invasiveness and postoperative outcomes. Further data informing the potential extent and complexity of an ASD surgery may help patients and surgeons better prepare for these major operations. Patients with preoperative CM can expect longer and more complex procedures the worse their CVA is, and the clinical team can make necessary adjsutments, including anesthetic selection, preparation of blood products, and implementation of antifibrinolytics. Surgeons can communicate the anticipated increase in operative time and blood loss with CM to their anesthesia colleagues, and potentially plan for intensive care unit monitoring. Furthermore, the void in coronal alignment goals may be a contributing factor to these findings. It is possible that clearer guidance on coronal alignment threshold, both in terms of CVA and maximum Cobb angle, may help optimize surgical plans and decrease the morbidity of these operations.
The present study is not without limitations. First, as a retrospective single-center study with 2 surgeons involved, differences may exist when including additional centers and surgeons with varying approaches and techniques. There were 2 surgeons who made the preoperative decision-making, which may limit the generalizability of our results. It is common practice at our hospital to employ an all-posterior approach, and lateral, oblique, or anterior approaches may yield different findings. To that end, larger, prospective studies are needed to assess the validity and applicability of our findings. Second, postoperative outcomes measured here were limited to overall complications, reoperations, and readmissions. Future research should examine the relationship between alignment groups and more granular complications, as well as the impact on patient-reported outcomes. Particularly understudied are patients with CCSM, and this difficult subset of patients should be an area of future work.
CONCLUSION
In patients undergoing ASD surgery, preoperative alignment led to significantly different surgical invasiveness and operative complexity. The CM group had more instrumented levels, underwent more PCOs, and had more TLIFs than the SM group, and the CCSM group had TLIFs performed more often and higher blood loss than the SM group. The amount of CM (CVA) held a stronger linear association with 3 operative complexity variables than amount of SM (SVA). Both SM and CCSM patients had the highest rate of readmission and reoperation. Together, these findings suggest that CM is significantly associated with increased invasiveness and complexity in ASD surgery.
Notes
The authors have nothing to disclose.