






INTRODUCTION
Cervical deformity is a complex topic, and despite its importance, the main focus in the spine literature during the past decade has been mainly on thoracic and lumbar deformities [1,2].
Cervical spine represents the connection area between the head and the trunk, it has therefore an important flexibility in order to orientate the head in different directions and also maintain horizontal gaze. In fact, any change that may occur in cervical spine sagittal parameters, happens in order for the person to maintain the horizontal gaze and be able to look forward [3].
When we study the cascade of events involving spinopelvic sagittal alignment, cervical spine mainly interacts with its adjacent areas, the craniocervical junction and the thoracic spine, as it actually responds to any change that occur in those adjacent areas. For example, if thoracic kyphosis decreases as a compensation to degenerative hypolordosis, this will lead to a decrease in the C7 slope, resulting in cervical hypolordosis or even cervical kyphosis [4]. In case of a major thoracolumbar or thoracic kyphotic deformity, the positive sagittal malalignment will lead to an increase in the C7 slope, resulting in cervical hyperlordosis [5,6].
The close interaction between the cervical spine and the thoracic spine enables the identification of 2 types of cervical deformities:
(1) Cervical deformity arising from inside the cervical spine and related to either degenerative, traumatic, iatrogenic or congenital cervical pathologies. In such category, the problem will need to be dealt with inside the cervical spine by performing the surgical correction techniques such as diskectomies, corpectomies, or osteotomies through either single (anterior or posterior) or combined approaches [7-9].
(2) Cervical deformity arising from outside the cervical spine and related to a spinal malalignment adjacent to the cervical area, mainly in the upper thoracic spine such as posttraumatic deformity or proximal junctional kyphosis. The cervical deformity is in fact a compensatory deformity in order for the patient to maintain the horizontal gaze. In this category, the problem will need to be dealt with outside the cervical spine in the adjacent upper thoracic area [10,11].
In this article, we will focus on the latter situation when cervical deformity arises from outside the cervical spine, managing it by performing a pedicle subtraction osteotomy (PSO) in the upper thoracic area. Restauration of proper sagittal and coronal alignment will indirectly correct the cervical deformity to a properly aligned cervical spine.
PREOPERATIVE CONSIDERATIONS
Rigid thoracic hyperkyphosis or kyphoscoliosis may be the result of different pathologies such as, neurofibromatosis (NF), proximal junctional kyphosis (in a previously operated patient), posttraumatic kyphosis, and degenerative disease.
Positive sagittal malalignment created by thoracic hyperkyphosis usually leads to intractable back pain, and also neck pain related to the compensatory cervical deformity in hyperlordosis.
A full radiographic workup should be performed including full spine anteroposterior and lateral radiographs to assess global spinal alignment, a computed tomography (CT) scan with sagittal and coronal reconstructions, and magnetic resonance imaging (MRI) to rule out any congenital anomalies such as dural ectasia or rib-head dislocation in NF patients.
When conservative management including analgesia and physiotherapy have failed, surgical management remains the only valid treatment option. Different osteotomy techniques may be cited. Posterior column osteotomies or Ponte osteotomies are ideally performed in patients with adequate disc height and residual flexibility within the intervertebral disc, in addition correction is limited to the sagittal plane, therefore they are of limited utility in rigid thoracic hyperkyphosis. Posterior vertebral column resection is a very efficient technique for the correction of rigid kyphotic deformity, nevertheless it remains a very demanding procedure with high risks of complications, including significant blood loss and neurological deficit [12]. Three column osteotomy or pedicle subtraction osteotomy is a technically demanding technique, but nevertheless considered safer than the previously aforementioned vertebral column resection (VCR), it enables correction of the rigid deformity in both sagittal and coronal planes and has been advocated as an ideal technique for the upper thoracic area [11,13,14]. The following paragraph will describe in details the different steps of performing an upper thoracic PSO (between T1 and T5).
STEP-BY-STEP DESCRIPTION OF THE PROCEDURE
(1) The patient is placed in a prone position with the head fixed in a Mayfield frame. The thoracic bolsters should be placed slightly more distally to accommodate the shape of the proximal thoracic spine. Furthermore, the head position will most likely lie below the level of the chest and adequate space beyond the head and below the face is important. This may be helped by a slight reverse Trendelenburg position.
(2) The surgical procedure is performed with intraoperative neuromonitoring (motor and somatosensory evoked potentials). Systolic blood pressure of greater than 100 mmHg is rigorously maintained throughout each case to ensure adequate spinal cord perfusion.
After posterior approach, midline paravertebral exposure and facetectomies are performed, and intraoperative navigation images are obtained.
While pedicle screws are inserted mostly using the free-hand technique for the vertebrae caudal to the PSO level, proximal thoracic and cervical pedicles tend to be more difficult in the presence of severe kyphosis; thus, accuracy is improved with navigation. Navigation is also beneficial during this procedure for placing implants in old fusion masses or abnormal osseous morphology and for identifying the limit of the depth of bone resection during the osteotomy procedure.
After all screws are inserted, early preparation of the precontoured rods is advised in order for them to be ready to avoid losing time later on when the reduction step is reached (ongoing bleeding), or in case the surgery has to be finished quickly for any reason.
(3) The posterior aspect of the ribs at the level of the vertebra undergoing the PSO is exposed through the same incision so as to remove approximately 5 cm of rib including the rib head on both sides (Supplementary video clip 1). Remaining extrapleural is difficult, and frequently a small pleural perforation can occur. A chest radiograph may be performed in the recovery room postoperatively and seldom a chest drain may be inserted if hemothorax is evident radiographically. Bilateral and partial costectomies allow good visualization of the vertebral bodyŌĆÖs lateral walls and the posterior vertebral wall. This large resection will avoid spinal cord mobilization maneuvers during the osteotomy procedure. It is advisable to remove each rib section en bloc as the free rib end (once cut laterally) can be mobilized to aid hemostasis as it is dissected medially, with the aid of a Penfield dissector from the costotransverse and costovertebral joints.
(4) Exposure of the lateral vertebral body wall is carried out bilaterally with a sharp Cobb dissector and a cellulose mesh (Surgicel, Ethicon, Sommerville, NJ, USA) is applied to the segmental vessels, which lie at the equator of the vertebra. Vertebral body resection is made from the lateral wall, through the pedicles as the spinal canal is finally exposed. After posterior element and pedicle resections, the lateral vertebral body wall cuts are made with straight osteotomes in a precise wedge, based on the desired degree of closure (Supplementary video clip 2). The distal cut is made below the pedicle and the proximal cut is just above the inferior endplate of the cephalad vertebra to the osteotomy level (i.e., Schwab osteotomy type 4). The resection depth (apex of the wedge) is controlled by the navigation to ensure that the wedge apex is 1 cm before the anterior vertebral body wall. No temporary rod is placed during the osteotomy. The posterior wall is removed with 45┬░ angulated pituitary forceps. The forcepsŌĆÖ jaws are opened outside the vertebra, and the upper jaw is inserted carefully between the anterior dura and the posterior wall. Then the bone is pushed anteriorly into the vertebra. Removing the upper intervertebral disc allows a higher degree of correction and increases the probability of fusion (bone-to-bone contact). In the disc space, the same posterolateral technique is used to approach the resection of the posterior annulus and disc.
(5) Final correction is achieved by simultaneous internal and external maneuvers (Supplementary video clip 3). An experienced operator (outside of the surgical field) who is familiar with the workings of the Mayfield frame in this indication is best placed so that they can steadily maintain the Mayfield frame as an assistant loosens the table attachments. Two precontoured cobalt chrome rods connected by a domino are applied across the PSO site either in one block from proximal to distal or separately. The head and neck are then extended to create closure of the osteotomy with rod insertion in the distal screws or telescoping of the rods at the level of the domino. If the kyphosis is such that the proximal and distal rods do not meet before correction, then the rods are applied distally and as the head is lifted, the rods are guided into the proximal screws (cantilever bending). These combined maneuvers allow posterior closing of the wedge site, ultimately leading to a smooth correction while avoiding spinal cord trauma at the osteotomy level. Compression on the convex site of a coronal deformity allows for an asymmetric closure and a coronal plane correction if needed. During the correction maneuver, it is very important to pay attention to neuromonitoring; signal changes must guide the surgeon to stop or alter the technique and correction. Once correction is achieved, the Mayfield frame is fixed in place before starting decortication and wound closure. A postoperative Philadelphia cervical collar is worn for 3 months by all patients. Secondary surgery to perform an anterior graft by thoracotomy is usually not necessary.
RESULTS
Proximal upper thoracic PSO performed for upper thoracic kyphosis and compensatory cervical deformity has been reported to achieve good correction in the sagittal plane. In a series reported by Obeid et al. [11], segmental kyphosis and thoracic kyphosis both significantly decreased by 26.6┬░ and 29.5┬░, respectively, which induced a reduction of the C1ŌĆō7 cervical lordosis and the C7 slope by 20┬░ each. A significant correlation was found between the reduction of thoracic kyphosis and the reduction of C1ŌĆō7 lordosis. Average operative time was 291 min, blood loss was 1,650 mL, and hospital stay was 13.8 days. There were no transient or permanent neurological complications, and no pseudarthrosis reported.
The use of the Mayfield frame and the preservation of the anterior vertebral wall provide good stability during the resection and correction maneuvers. Furthermore, the use of simultaneous internal and external correction maneuvers allows for a progressive and safe correction which decreases the neurological risks.
If the lower cervical spine is included in the construct, and in order to avoid any iatrogenic stenosis of the intervertebral foramens, it is advised to check on preoperative MRI and CT scans on any pre-existing stenosis in order to decompress it during the surgery, otherwise decompression is not required but the exiting nerve roots may be eventually controlled intraoperatively before the final fixation. No cases of cervical radiculopathy occurred in our patients.
Fixation is usually extended 3 levels proximally to the osteotomy level, rarely 2 levels in case of T2 PSO in order to stop at C7 (with strong pedicular purchase) and avoid fixing C6.
Upper thoracic PSO can be asymmetrical and may also correct the deformity in both coronal and sagittal planes when needed [15]. Use of the domino on the convex side will enable good asymmetrical correction with the compression effect spread on all the proximal and distal screws simultaneously.
It should be mentioned that in severe cases with importantly deformed apical vertebra, the limit between a PSO and a VCR may become less obvious as nonintentional removal of the lower disc may occur given the difficult anatomical configuration. In such a case, the osteotomy becomes rather a resection, and the use of a mesh cage in order to restore the anterior column height and avoid overshortening with eventual neurological compromise is advisable.
Correction of the upper thoracic deformity imposes cervical spine adaptation, given the close relationship between the 2 regions, and therefore an automatic correction of the cervical deformity.
ILLUSTRATIVE CASES
1. Case 1 (Corresponding to the Video Demonstration)
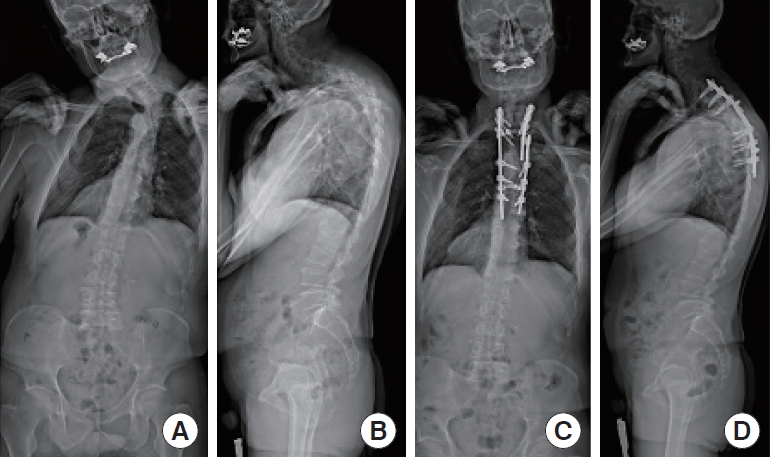
A 58-year-old male presented with a neck deformity because of a posttraumatic cervicothoracic kyphoscoliosis. Preoperative local kyphosis was 85┬░, cervical lordosis 66┬░, and right cervicothoracic scoliosis 48┬░. He underwent an asymmetrical PSO at the level of T5. Local kyphosis was corrected to 48┬░, cervical lordosis to 31┬░, and scoliosis to 10┬░ (Fig. 1AŌĆōD).
2. Case 2
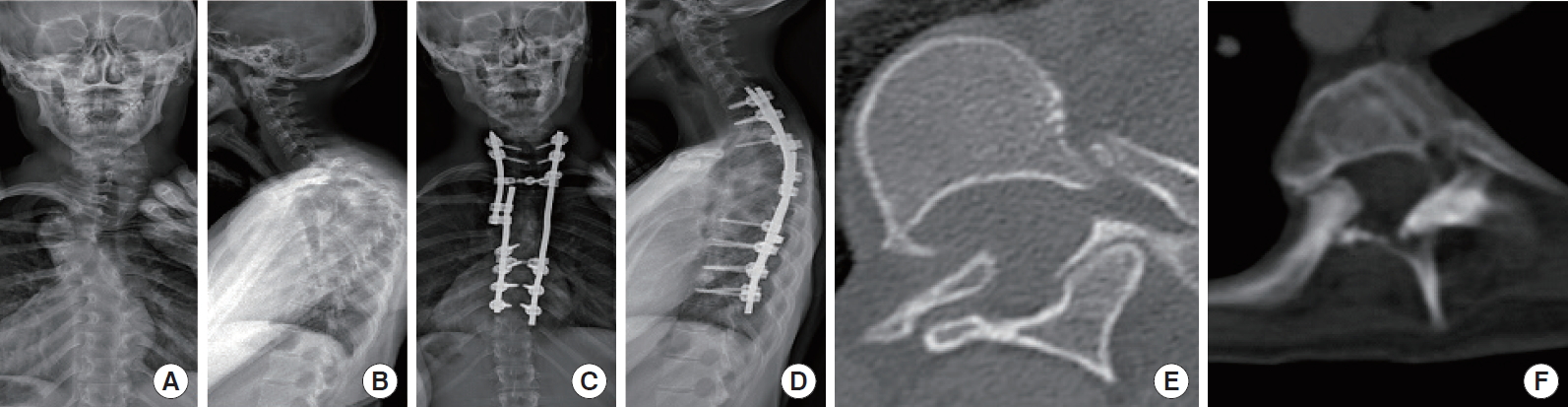
A 26-year-old female previously operated for an adolescent idiopathic scoliosis with anterior and posterior instrumentation. She presented iatrogenic proximal junctional kyphosis with 86┬░ between T2 and T6 and a compensatory cervical hyperlordosis of 48┬░. She underwent a PSO at the level of T5 correcting the thoracic kyphosis to 54┬░ and the cervical lordosis to 18┬░ (Fig. 2AŌĆōF).
3. Case 3
A 17-year-old female with cervicothoracic kyphoscoliosis in the context of NF. Preoperative local kyphosis was 45┬░, cervical lordosis 18┬░, and left cervicothoracic scoliosis 38┬░. She underwent a PSO at the level of T4. Local kyphosis was corrected to 15┬░, cervical lordosis to 2┬░, and scoliosis to 6┬░ (Fig. 3AŌĆōF).
RISKS, COMPLICATIONS, AND THEIR PREVENTION
ŌĆó Poor fixation proximally to the osteotomy. This is why in such cases, navigation is important in order to guarantee strong pedicle screws insertion and avoid hooks.
ŌĆó Inadequate correction maneuvers. Performing the simultaneous external/internal maneuvers during reduction decrease the stress on the pedicle screws and spinal cord with a smooth reduction from proximal to distal (head and rods). In addition, the domino compression spreads the loads on all the screws simultaneously.
ŌĆó Dural kinking in case of revision surgery with inadequate decompression around the osteotomy. Proper scar removal and wide laminectomy especially at the level proximal to the osteotomy may decrease such a risk. In addition, insertion of a mesh cage in the osteotomy gap may be advised in case of important shortening with risks of altered motor evoked potentials, as it would help in restoring the vertebral height acting as an anterior column support and stabilizer.
ŌĆó Spinal cord injury. Leaving 5 to 10 mm of the anterior cortex enables maintaining the stability of the osteotomized level, it acts as an anterior tension band that would guide the anterior column during the correction maneuvers, avoiding the need for temporary rod, and avoiding column translation with potential cord injury.
ŌĆó Excessive bleeding. This may be prevented by performing meticulous dissection, good hemostasis in the epidural space, pedicle screws insertion with the free-hand technique distally to the osteotomy to shorten the surgical time and preparing the rods before even opening the canal for them to be ready for the reduction as soon as the osteotomy is performed.
ŌĆó In order to achieve a high posterior fusion rate, it is advised to cover the osteotomy area (where the major posterior bone defect is present) with gelfoam or a sealant to protect the dura and add on top of it parts of the ribs that have been removed and place same in a longitudinal fashion bridging the defect from the proximal intact lamina to the distal intact lamina. With this technique, and after bony bed freshening, continuous bone graft may be placed in the central posterior area of the spine from the proximal to the distal part of the whole construct.
ŌĆó A specific risk inherent to NF patient should be mentioned, as rib-head dislocation may be present and may increase the risk of cord injury. Preventing the aforementioned risk comes first with a complete depiction of the anatomy preoperatively with a CT scan to detect such a dislocation, and secondly intraoperatively where it is advised to remove it. Navigation may help in checking the complete rib-head removal and satisfying spinal canal diameter.
CONCLUSION
Cervical deformity arising from upper thoracic malalignment is a compensatory deformity that illustrates the close relationship between the proximal thoracic spine and the cervical spine, with the aim of maintaining the horizontal gaze by increasing the cervical lordosis. Such a deformity is dealt with by treating the problem at its origin outside the cervical spine by performing a PSO in the upper thoracic spine.
Proximal thoracic PSO is a safe and effective, albeit technically demanding surgical procedure for the management of cervicothoracic deformity.











")













