







INTRODUCTION
Cervical disc replacement (CDR) has been established as a safe and effective surgical option for patients with degenerative disc disease who fail nonoperative management [1-8], with numerous studies demonstrating similar or superior outcomes in various measures, including adjacent segment pathology, patient-reported outcome measures (PROMs), rate of dysphagia, patient satisfaction, rate of revision and secondary surgeries, and cost-effectiveness compared to anterior cervical discectomy and fusion (ACDF) [9-18].
Although the clinical benefits of CDR have been well-established in literature, the use of this technique in patients with nonlordotic cervical sagittal alignment is not well-established. Currently, there is lack of widely accepted knowledge regarding the effectiveness of CDR on correcting and maintaining sagittal alignment. Furthermore, earlier studies had reported postoperative kyphosis as a potential adverse outcome of CDR [19,20]. Therefore, there is concern that the use of this technique in nonlordotic patients may worsen the alignment and negatively impact clinical outcomes.
Recent studies have reported successful correction of sagittal alignments following CDR [21-23], but only few have analyzed the effect of nonlordotic preoperative sagittal alignments on both clinical and radiographic outcomes. Thus, the purpose of this study was to evaluate the impact of nonlordotic segmental and regional sagittal alignment on clinical and radiographic outcomes following CDR.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board (IRB) of Hospital for Special Surgery (IRB No. 2019-0018).
1. Patient Population
This was a retrospective review of prospectively collected data of a 3-surgeon cohort of patients who underwent surgery at a single academic institution between February 2016 and February 2020. Consecutive patients who underwent primary elective 1- or 2-level CDR for cervical discogenic myelopathy or radiculopathy were included. Patients who underwent revision surgery (n =1) or concomitant fusion (n =6) were excluded. Patients who did not have preoperative radiographic imaging available in the Picture Archiving and Communications System (PACS) were also excluded (n =4).
All surgeries were performed using the Smith-Robinson approach, which is described extensively in previous literature [24-26]. All surgeries utilized the Mobi-C implant (Zimmer Biomet, Warsaw, IN, USA). Implant size was determined intraoperatively by the operating surgeon, and implant height for all patients included in this series was either 5 mm or 6 mm.
2. Data Collection
Patient demographics and comorbidity burden, including age, sex, race, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification, age-adjusted Charlson Combined Comorbidity Index (age-adjusted CCI), were obtained from electronic medical records. Surgical details, including number of levels and level of surgery, and postoperative complications were also obtained from the electronic medical records. PROMs, including Neck Disability Index (NDI), visual analogue scale for neck and arm pain (VAS neck and VAS arm), and Short Form-12 physical and mental health scores (SF-12 PHS and SF-12 MHS), were collected prospectively as standard of care [27]. PROMs collected preoperatively, and postoperatively at follow-up of < 6 months and ≥ 6 months were included for analysis.
All data were collected and managed using REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center for Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384. REDCap is a secure, web-based software platform designed to support data capture for research studies [28,29].
3. Radiographic Measurements
Measurements of all radiographic parameters were performed using the hospital’s PACS by researchers not involved in patient care. Lateral standing plain radiographs (neutral position with the patient’s eyes gazing forward) were obtained preoperatively and postoperatively at < 6 months and ≥ 6 months. These were used to measure segmental Cobb angle, C2–7 Cobb angle, cervical sagittal vertical axis (cSVA), cranial tilt, and T1 slope. Sagittal alignment parameters were measured using previously established methods [30,31]. Segmental Cobb angle at the level of surgery was defined by the Cobb angle between the superior endplate of the cranial vertebral body and the inferior endplate of the caudal vertebral body. C2–7 Cobb angle was defined by the Cobb angle between the inferior endplates of C2 and C7. cSVA was defined as the distance from the C2 plumb line to the posterior end of the superior endplate of C7. Cranial tilt was defined as the angle formed between the line from the tip of the dens to the center of the superior endplate of T1 and the SVA from the superior endplate of T1 [30]. T1 slope was defined as the angle between the horizontal plane and the superior endplate of T1.
For segmental Cobb angle and C2–7 Cobb angle, a lordotic angle was designated as a negative angle (< 0°), and nonlordotic as a positive angle (> 0°). Instead of using the term “kyphotic” to denote Cobb angles > 0°, we used the term “nonlordotic,” as none of our patients had significant cervical kyphotic deformities. Based on these measurements, patients were divided into 3 cohorts: (1) neutral/lordotic segmental and C2–7 Cobb angle (cohort “L”), (2) nonlordotic segmental Cobb angle, lordotic C2–7 Cobb angle (cohort “NL-S”), and (3) nonlordotic segmental and C2–7 Cobb angle (cohort “NL-SC”).
4. Statistical Analysis
Continuous variables are summarized as mean ±standard deviation and categorical variables are summarized as N (% within group). Chi-square or Fisher exact test was used to compare categorical variables. One-way analysis of variance or Kruskal-Wallis test was used to compare normally and nonnormally distributed continuous variable, respectively, among the 3 groups. Post hoc analyses were performed to determine which pairwise comparisons were statistically significant. Paired samples t-test or Wilcoxon signed-rank test was used to assess changes in normally and nonnormally distributed continuous variables, respectively within each group. For any baseline demographics/characteristics that were significantly different among the 3 cohorts, multiple regression analyses were performed to control for their impact on outcomes.
Statistical significance was set at p-value < 0.05. Analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Patient Characteristics
Of the 109 patients that met the inclusion/exclusion criteria, 4 patients with nonlordotic cervical alignments but lordotic segmental angles were excluded due to this cohort’s small sample size. Of the 105 patients included, 66 underwent 1-level CDR and 39 underwent 2-level CDR. There were 37 patients in cohort L, 30 patients in cohort NL-S, and 38 patients in cohort NL-SC. Patient demographics and baseline characteristics are summarized in Table 1. There was a statistically significant difference in age (p=0.015) among the 3 groups, with post hoc analysis showing that cohort L was significantly older than cohort NL-SC (mean age: 45.73 years vs. 39.76 years, p=0.016). There were no significant differences in gender, race, BMI, ageadjusted CCI, or ASA physical status classification. There were no significant differences in the number of levels or the level of surgery among the 3 cohorts. There were no significant differences in postoperative complications.
2. Radiographic Parameters
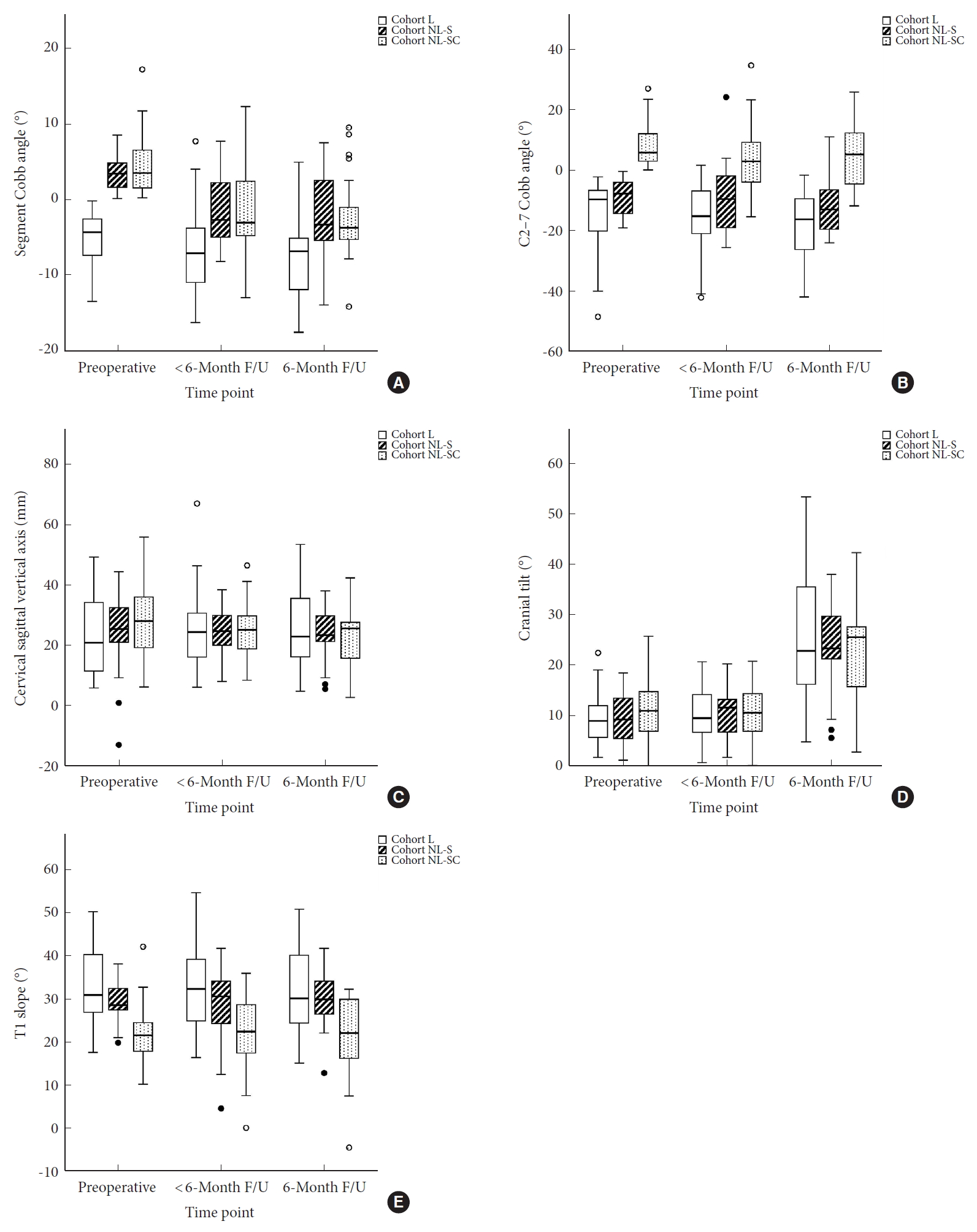
All patients had x-rays obtained preoperatively and at <6-month follow-up, with radiographs obtained at a mean of 77±31 days after surgery. At ≥ 6-month follow-up, 73 patients (70%) had radiographs available for measurement, with radiographs obtained at a mean of 358±238 days after surgery. For the entire cohort, preoperative segmental lordosis ranged from -13.5° to 17.2° (25th to 75th percentile: -3.5° to 3.75°), and C2–7 lordosis ranged from -48.6° to 27.0° (25th to 75th percentile: -12.2° to 3.4°). Sagittal alignment parameters are shown in Fig. 1.
1) Segmental Lordosis
As seen in Table 2, a statistically significant difference was seen in the preoperative segmental Cobb angle among the 3 groups (p<0.0001). Post hoc analysis demonstrated that cohort L had a lordotic segmental Cobb angle preoperatively (-5.28 ±3.58), which was significantly different from the nonlordotic segmental Cobb angles seen in cohort NL-S (3.54 ±2.34, p < 0.0001) and NL-SC (4.46±3.66, p<0.0001), with no significant difference between NL-S and NL-SC (p=1.000). As seen in Table 3, all cohorts showed a statistically significant gain in lordosis at follow-up of < 6 months (p=0.007 for cohort L, p<0.0001 for cohorts NL-S and NL-SC) and ≥ 6 months (p=0.040 for cohort L, p<0.0001 for cohorts NL-S and NL-SC). Furthermore, cohorts that were nonlordotic preoperatively (NL-S and NL-SC) had greater gains in lordosis compared to the preoperatively lordotic (L) cohort (p<0.0001 for both), and the mean segmental Cobb angle for these cohorts changed from a nonlordotic angle preoperatively to a lordotic angle postoperatively ( < 6-month follow-up: NL-S=-1.62±4.22 and NL-SC=-1.54±5.79; ≥ 6-month follow-up: NL-S=-2.36±5.48 and NL-SC=-2.45±5.14). Despite this larger gain in lordosis by the NL-S and NL-SC cohorts, the postoperative segmental Cobb angle in cohort L was significantly more lordotic (< 6-month follow-up=-7.19±5.34, ≥ 6-month follow-up=-6.93±5.21) than either of these cohorts at the < 6-month (p<0.0001) and ≥ 6-month follow-ups (p<0.0001).
2) C2–7 Cobb angle
As seen in Table 2, a statistically significant difference was seen in the preoperative C2–7 Cobb angle among the 3 groups (p<0.0001), with post hoc analysis demonstrating that cohort NL-SC had a nonlordotic C2–7 Cobb angle preoperatively (8.04±6.89), which was significantly different from the lordotic Cobb angles seen in cohort L (-14.57±11.54, p<0.0001) and NL-S (-8.80 ±5.70, p < 0.0001), with no significant difference between L and NL-S (p=0.669). Cohorts L and NL-S maintained their lordosis postoperatively (p> 0.05 for change in Cobb angle). As seen in Table 3, Cohort NL-SC showed a statistically significant gain in lordosis at follow-up of < 6 months (p=0.006) and ≥ 6 months (p=0.005). Cohorts NL-S also showed a statistically significant gain in lordosis at follow-up of ≥ 6 months (p=0.017). However, despite significant improvement in the C2-C7 Cobb angle, Cohort NL-SC did not achieve lordotic cervical alignment postoperatively (< 6-month follow-up=3.89±10.46; ≥ 6-month follow-up=4.06±10.37), and was significantly less lordotic than either of the other 2 cohorts at the <6 months (cohort L=-16.30±11.65; cohort NL-S=-9.58±11.05) and ≥ 6-month follow-ups (cohort L =-18.70 ±11.81; cohort NL-S =-11.84±9.12).
3) T1 slope
As seen in Table 2, a statistically significant difference was seen in the preoperative T1 slope among the 3 groups (p<0.0001), with post hoc analysis demonstrating that cohort NL-SC had a significantly smaller T1 slope preoperatively (21.91±6.72), compared to cohort L (32.63±8.64, p<0.0001) and NL-S (29.18±4.38, p<0.0001), with no significant difference between the latter 2 (p=0.140). There were no significant changes in the T1 slope at either follow-up in any cohort. The preoperative differences in T1 slope remained postoperatively.
4) cSVA
No significant difference in cSVA was seen among the 3 cohorts at any time-point (Table 2). Cohort NL-SC demonstrated a significant improvement in cSVA at the < 6 months (mean change: -3.56±8.62, p=0.017) and ≥ 6 months (mean change: -4.46±10.15, p=0.042) follow-up (Table 3). A statistically significant difference was seen among the 3 cohorts in the amount of change in cSVA at the < 6-month follow-up (p=0.013), with post hoc analysis demonstrating cohort L showed no significant change in cSVA compared to a statistically significant decrease in cSVA for cohort NL-SC (mean change=1.48±8.06 for cohort L vs. -3.56±8.62 for cohort NL-SC, p=0.012). No difference was seen at the ≥ 6-month follow-up.
5) Cranial tilt
No significant difference in cranial tilt was seen among the 3 groups at any time-point (Table 2), and no significant change was seen from pre- to postoperatively in any group at either time-point. However, a significant difference was seen among the 3 cohorts in the amount of change in cranial tilt at the < 6-month follow-up (p=0.036), with post hoc analysis demonstrating a significant difference between cohort L and cohort NL-SC (1.09±5.12 vs. -1.06±4.57, p=0.032) (Table 3). No difference was seen at the ≥ 6-month follow-up.
3. PROMs
Preoperatively, 94 patients (90% of total patients) had completed PROMs. At < 6-month and ≥ 6-month follow-up, 92 patients (88%) and 72 patients (69%), respectively, had completed PROMs. PROMs at the < 6-month follow-up were completed at an average of 76±27 days after surgery and those at the ≥ 6 months’ time-point were completed 305 ±194 days after surgery. PROMs are shown in Fig. 2. There were no significant differences among the 3 groups in preoperative PROMs, postoperative PROMs or change in PROMs at any time-point, except for VAS neck at < 6-month follow-up (p=0.023), with post hoc analysis showing that cohort NL-S had significantly higher VAS neck than cohort NL-SC (mean VAS neck: 3.33 vs. 1.76, p=0.027) (Table 4). This difference was not seen at ≥ 6-month follow-up. All 3 cohorts showed statistically significant improvements in NDI, VAS neck, and VAS arm at both <6-month and ≥6-month follow-ups (Table 5). Cohorts L and NL-SC also demonstrated significant improvements in SF12-MHS at < 6-month follow-up, with cohort L showing significant improvement in SF12-MHS at ≥ 6-month follow-up. Cohort NL-SC also showed significant improvements in SF12-PHS at both follow-ups.
Linear regression analysis showed that age was not significantly associated with any radiographic or patient-reported outcomes (p> 0.05).
4. Case Examples
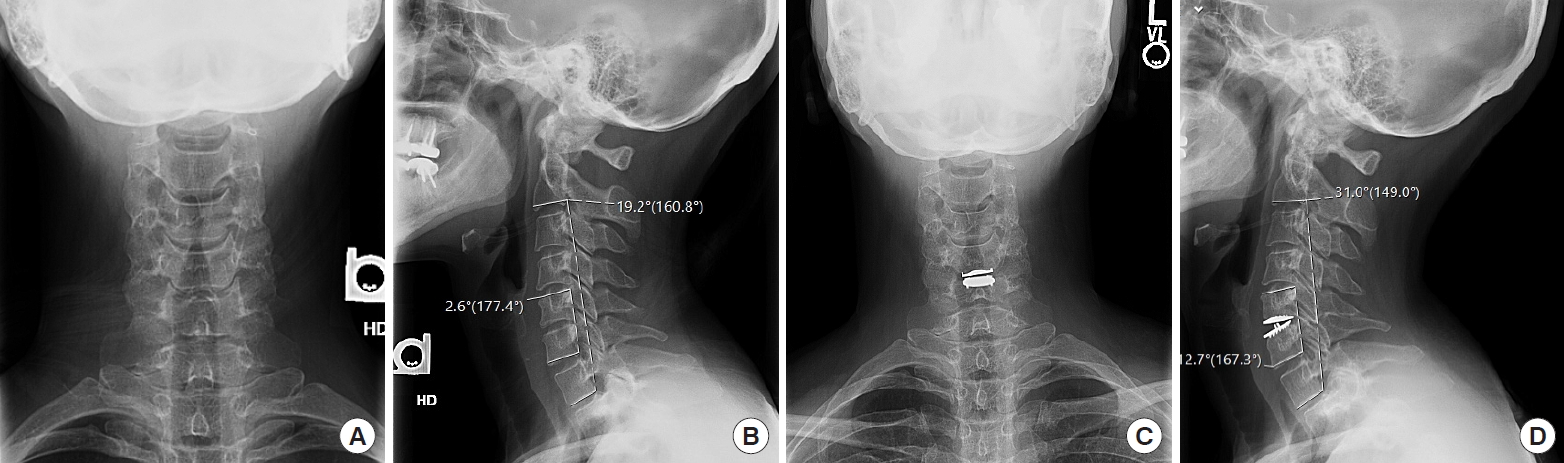
1) Case #1: neutral/lordotic segmental Cobb angle and C2–7 Cobb angle
A 42-year-old female presented with radicular right arm pain for 2 years, which had worsened in the 2 months prior to presentation. The patient had attempted physical therapy, acupuncture, nonsteroidal anti-inflammatory drugs (NSAIDs), and muscle relaxants with little improvement in symptoms. She had also received numerous epidural steroid injections over the past 2 years, which provided temporary pain relief but the duration of pain relief between epidural injections had decreased from 1 year to < 3 months. Preoperative NDI was 32, VAS neck was 10, and VAS arm was 10. Preoperative segmental Cobb angle was -2.6° and C2–7 Cobb angle was -19.2°. The patient was diagnosed with C5C6 left severe foraminal stenosis with radiculopathy secondary to a disc osteophyte complex and underwent C5C6 cervical disc arthroplasty without complications. Operative time was 97 minutes and estimated blood loss was 70 mL. The patient was discharged 26 hours after surgery and there were no postoperative complications. At the last follow-up, NDI, VAS neck, and VAS arm were 0; the segmental Cobb angle was -12.7° and the C2–7 Cobb angle was -31.0°. Anteroposterior (AP) and lateral radiographs at the preoperative time-point and at the last follow-up are shown in Fig. 3.
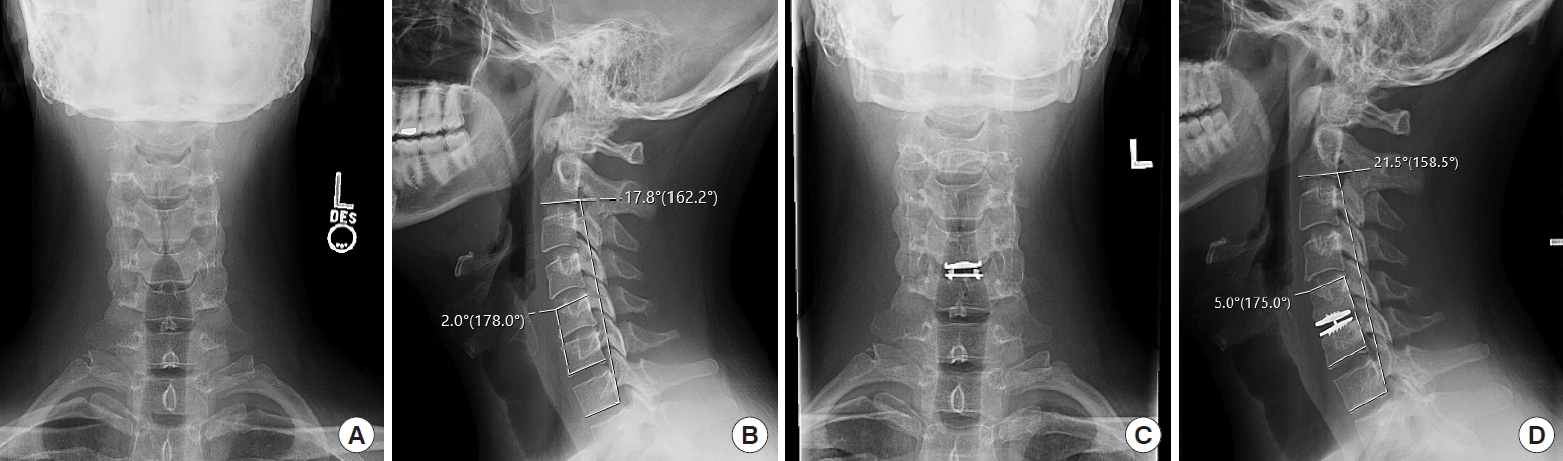
2) Case #2: nonlordotic segmental Cobb angle, lordotic C2–7 Cobb angle
A 35-year-old male presented with right-sided neck, periscapular and trapezial pain for the past 6 years, along with right arm weakness in the 2 months prior to surgery. The patient had attempted physical therapy and NSAIDs with no relief of symptoms. Preoperative NDI was 40, VAS neck was 7, and VAS arm was 2. Preoperative segmental Cobb angle was 2.0° and C2–7 Cobb angle was -17.8°. The patient was diagnosed with C5C6 herniated nucleus pulposus with radiculopathy and underwent C5C6 cervical disc arthroplasty without complications. Operative time was 89 minutes and estimated blood loss was 50 mL. The patient was discharged 24 hours after surgery and there were no postoperative complications, except for urinary retention requiring 1-time catheterization. At the last follow-up, NDI was 20, VAS neck was 4, and VAS arm was 2; segmental Cobb angle was -5.0° and C2–7 Cobb angle was -21.5°. AP and lateral radiographs at the preoperative time-point and at the last follow-up are shown in Fig. 4.
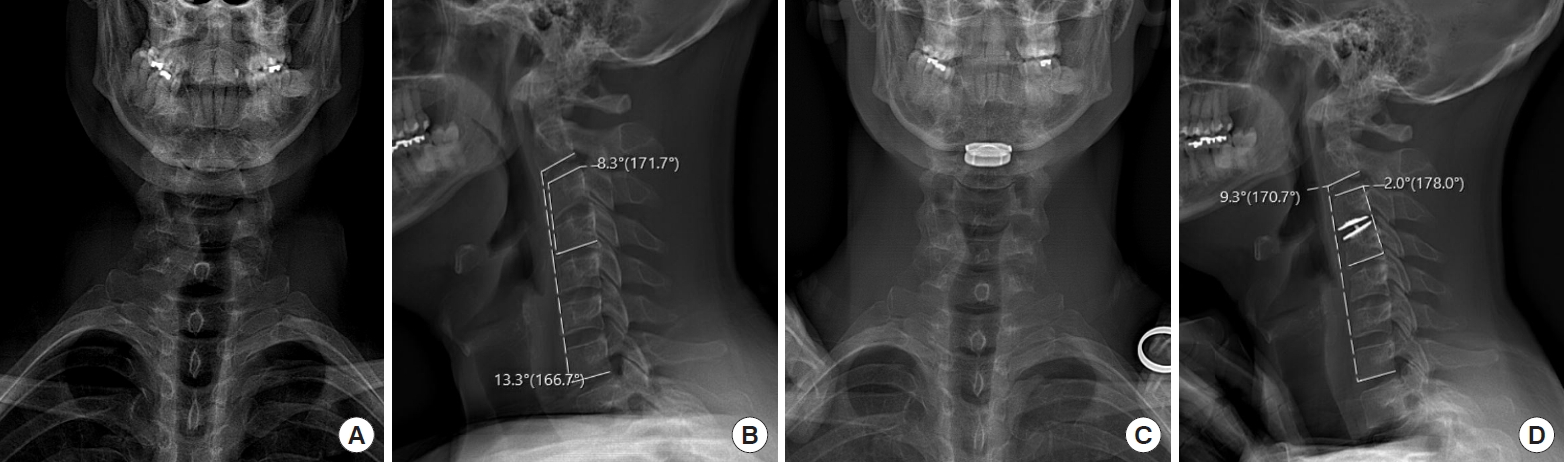
3) Case #3: nonlordotic segmental Cobb angle and C2–7 Cobb angle
A 45-year-old male presented with neck pain and radiating right arm pain for many years, which had acutely worsened in the 1 month prior to presentation. The patient had attempted physical therapy, muscle relaxants, oral steroids, and steroid injections with no relief of symptoms. Preoperative NDI was 36, VAS neck was 6, and VAS arm was 2. Preoperative segmental Cobb angle was 8.3° and C2–7 Cobb angle was 13.3°. The patient was diagnosed with C3C4 herniated disc with myelopathy and underwent C3C4 cervical disc arthroplasty without complications. Operative time was 47 minutes and estimated blood loss was 25 mL. The patient was discharged 4 hours after surgery and there were no postoperative complications. At the last follow-up, NDI, VAS neck, and VAS arm were 0; the segmental Cobb angle was -2.0° and the C2–7 Cobb angle was 9.3°. AP and lateral radiographs at the preoperative time-point and at the last follow-up are shown in Fig. 5.
DISCUSSION
CDR was first introduced as a motion-preserving surgery to reduce the biomechanical stress placed on adjacent segment levels associated with fusion surgeries. Over the past few decades, CDR has become increasingly utilized as an effective surgical technique to treat a variety of cervical spine pathologies [1,2]. With continued improvements in technology and devices, recent studies have demonstrated excellent medium- to long-term outcomes following CDR in properly selected patients [3-8]. Compared to ACDF especially, CDR has shown equally if not more superior outcomes in various measures: PROMs, patient satisfaction, rate of postoperative dysphagia, rate of revision surgeries or secondary surgeries, adjacent segment degeneration, and cost-effectiveness [9-18].
It is currently accepted that maintaining or increasing cervical lordosis is an important goal in the surgical treatment of cervical spondylotic myeloradiculopathy [32]. Initially, CDR was not known as a lordosis producing technique. Earlier studies had demonstrated issues of kyphotic angulation after insertion of certain disc prostheses [20,33]. However, more recent studies examining medium- to long-term outcomes following CDR have shown preservation or increase in cervical lordosis and correction of segmental kyphosis [21,22,34-36]. Anakwenze et al. [35] compared ACDF and CDR patients, and found significant improvements in cervical lordosis for both implants, with no significant difference between the 2 groups. Shi et al. [36] also compared ACDF and CDR patients and had found significant improvements in the overall sagittal alignment and functional spinal unit in both groups.
Though many studies have shown correction of sagittal alignments following CDR, the safety and effectiveness of this technique in patients with nonlordotic preoperative sagittal alignments is still not well-established. Chen et al. [37] found that patients with preoperative reducible kyphosis had significant improvements in sagittal alignments following CDR compared to those with irreducible kyphosis. The study also found that these patients with preoperative kyphosis had similar sagittal alignment to patients with preoperative lordosis at 2 years postoperatively [37]. Another study in 2013 from the same group compared clinical and radiographic outcomes after CDR or ACDF in patients with preoperative reducible kyphosis, and found no significant differences at 2 years postoperatively [38]. Based on the results of these 2 studies, the authors concluded that preoperative reducible kyphosis is not an independent contraindication for CDR. However, based on our literature review, no additional studies have examined this question, and there continues to be lack of widely accepted knowledge regarding the impact of nonlordotic alignment on outcomes of CDR. Based on the aforementioned studies and the authors’ own experience, off-label use of CDR to treat passively correctable nonlordotic preoperative sagittal alignment may be a safe technique resulting in improved postoperative patient-reported outcomes. The purpose of the current study was to further investigate the relationship between preoperative nonlordotic alignment and postoperative radiographic and clinical outcomes in patients undergoing an off-label use of CDR.
1. Radiographic Outcomes
1) Segmental Cobb angle
As expected, cohorts NL-S and NL-SC had nonlordotic segmental Cobb angles preoperatively, whereas cohort L had a lordotic preoperative segmental Cobb angle. All 3 cohorts gained lordosis following CDR, with greater amount of gain seen in the nonlordotic (NL-S and NL-SC) cohorts. However, despite this greater gain, these nonlordotic cohorts had less lordosis postoperatively compared to the neutral/lordotic cohort. These results are consistent with previous studies demonstrating maintenance or correction of segmental lordosis following CDR. In a 2-year clinical follow-up, Ahn et al. [21] demonstrated that patients that underwent C5–6 CDR with ProDisc-C artificial discs were able to achieve lordosis in the C5–6 Cobb angle postoperatively. In addition, Kim et al. [22] reported that following 1- or 2-level CDR, 13% of patients with preoperative segmental kyphosis achieved postoperative segmental lordosis. More recently, Chen et al. [37] had reported correction of preoperative segmental kyphosis in patients with reducible kyphosis following a single-level CDR. These findings and the results of our study indicate that CDR may be an effective treatment option for the improvement of segmental lordosis.
2) C2–7 Cobb angle
As expected, cohort NL-SC had a nonlordotic C2–7 Cobb angle preoperatively, whereas cohorts L and NL-S had lordotic alignment. Cohort NL-SC gained lordosis postoperatively; however, the alignment still remained nonlordotic at the later follow-up. Cohorts L and NL-S maintained their C2–7 lordotic alignment postoperatively. These results are consistent with previous studies demonstrating maintenance or correction of C2–7 lordosis following CDR. Park et al. [34] saw that patients undergoing a single-level CDR had significantly increased their C2–7 lordosis at > 2 years postoperatively. Kim et al. [22] had reported correction of preoperative overall cervical kyphosis in 33% of patients undergoing a single-level CDR. Chen et al. [37] had reported correction of preoperative C2–7 kyphosis in patients with reducible kyphosis following a single-level CDR. Taken together with the results of this study, CDR can effectively correct C2–7 lordosis.
3) cSVA
Even though there were no significant differences in cSVA among the 3 cohorts at all time points, cohort NL-SC saw significant improvements in their cSVA postoperatively, likely as a result of gain in C2–7 lordosis in this cohort allowing for a more upright head position.
Overall, CDR was able to generate segmental lordosis in all 3 cohorts, with greater lordosis generated in preoperatively nonlordotic cohorts. Despite this greater gain, postoperative segmental lordosis in preoperatively nonlordotic cohorts was still less than patients who had lordotic alignments preoperatively. CDR was able to improve C2–7 lordosis in those who were nonlordotic preoperatively, but this change was not enough to create a lordotic alignment. The cohorts that had lordotic C2–7 alignment preoperatively maintained their alignment postoperatively.
2. PROMs
Preoperative segmental or C2–7 alignment did not impact pre- or postoperative PROMs. All groups showed an improvement in NDI, VAS neck, and VAS arm from pre- to postoperative follow-ups, and there was no difference among the 3 cohorts in the amount of improvement achieved. These findings are in line with numerous previous studies showing improvements in various PROMs following CDR. A recent systematic review studied both short- and medium- to long-term outcomes following CDR and saw significant improvements in NDI, VAS scores, and SF-36 physical and mental scores [10]. Another recent systematic review found significant improvements in NDI following a 1-level CDR [39]. Specifically, in regards to patients with preoperative kyphosis, Chen et al. [37] had reported significant improvements in NDI and VAS in patients with preoperative reducible kyphosis at > 2 years postoperatively. In summary, patients with nonlordotic alignment preoperatively have significant improvements following CDR and have similar outcomes to those with lordotic alignment.
3. Strengths
This study evaluates the impact of nonlordotic segmental or regional alignment on the outcomes of CDR in a large prospective cohort of patients who underwent surgery consistent surgical technique and the same type of implant. While Chen et al. [37] included only 1-level CDR patients, our study included both 1- and 2-level CDR patients, allowing our findings to be more generalizable. Furthermore, Chen et al. [37] had stratified their patients based on global kyphosis only. Our study stratified patients based on not only global but also segmental lordosis, allowing us to more closely analyze the impact of each of these alignment parameters on postoperative outcomes. With a larger sample size, inclusion of 2-level CDR patients, and stratification based on both preoperative segmental and regional lordosis, our findings provide valuable information to surgeons who are considering 1- or 2-level CDR for patients with nonlordotic alignment.
4. Limitations
The study was a retrospective review of prospectively collected data, which inherently introduces selection bias. All surgeries were performed at a single academic institution, which potentially limits the external validity of the findings to a larger and more diverse population. Follow-up for radiographic and PROMs data was limited; thus, long-term outcomes could not be elucidated. Some patients were lost to follow-up and/or did not complete PROMs at their visit as a result of which complete radiographic and PROMs follow-up was not available for all patients. Additionally, all patients in our study received the same implant. Given the variety of implant designs available, it is not known whether these results are applicable to other types of implants. Lastly, the relatively young age of patients included in our study limit the generalizability of our results to an older population in which kyphosis may not be as passively reducible secondary to degenerative spondyloarthropathy associated with increasing age [40].
CONCLUSION
The results of our study show that patients without major kyphotic deformity who had nonlordotic segmental or C2–7 alignment demonstrated significant improvements in sagittal alignment and patient-reported outcome in the short-term follow-up following 1- and 2-level CDR. Specifically, CDR generated segmental lordosis regardless of preoperative alignment, with greater lordosis generated in those who were nonlordotic. It also showed improvement in cervical sagittal alignment, particularly C2–7 Cobb angle and cSVA in those with nonlordotic cervical alignment. Furthermore, preoperative alignment did not impact pre- or postoperative patient-reported outcomes, with all groups showing significant improvement after surgery. Thus, CDR has the potential to generate and maintain lordosis and improve patient-reported outcomes in the short-term, and can be an effective treatment option for patients with nonlordotic alignment. Further studies with longer follow-up are required to evaluate long-term outcomes such as sagittal alignment, implant failure, and need for revision surgery.











")













