




INTRODUCTION
Chondroma is a slowly growing benign cartilaginous neoplasm15). The most common sites are long bones of the hands and feet, but sometimes it ocurrs in ribs and pelvis, and rarely intracranial bones6). Although it is the most common benign tumor of bone, it is quite rare in the spine, especially the lumbar spine6,11). Chondroma in the spine comprises 3% of all chondromas and is commonly encountered in the thoracic spine10). Until now, only 15 cases of chondormas located in the lumbar spine have been reported. Although chondroma is generally asymptomatic, it may cause slowly developing neurologic deficit due to the mass effect of the lesion on the spinal cord or nerve roots4). Here, we report a rare case of chondroma in the lumbar spine presenting acute sciatica in a 47-year-old woman.
CASE REPORT
A 47-year-old woman presented with lumbago and severe left leg pain for 1 week. The patient had no trauma history or any experience of similar pain. The pain was aggravated by walking. The patient complained of severe radiating pain on left L3 sensory dermatome area and reported aggravation of leg pain at 20 degrees of hip flexion by SLRT. However, there was no motor weakness on neurological examination.
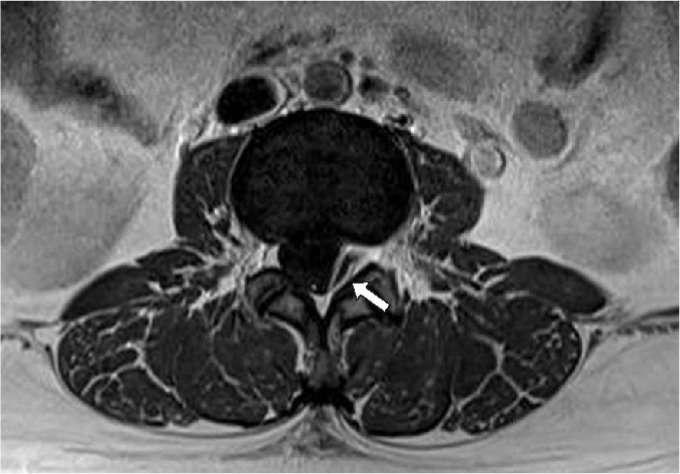
Plain films of the lumbar spine showed only loss of lordotic curvature. Computed tomography (CT) revealed no bony abnormality, such as osteolysis. Magnetic resonance imaging (MRI) demonstrated a plaque-appearing extradural mass which was located in the left and posterior spinal canal at L2-3 level. The lesion was homogeneous iso-SI on T1-WI, hypo-SI on T2-WI, and peripheral rim enhancement on a gadolinium enhanced MRI (Fig. 1).
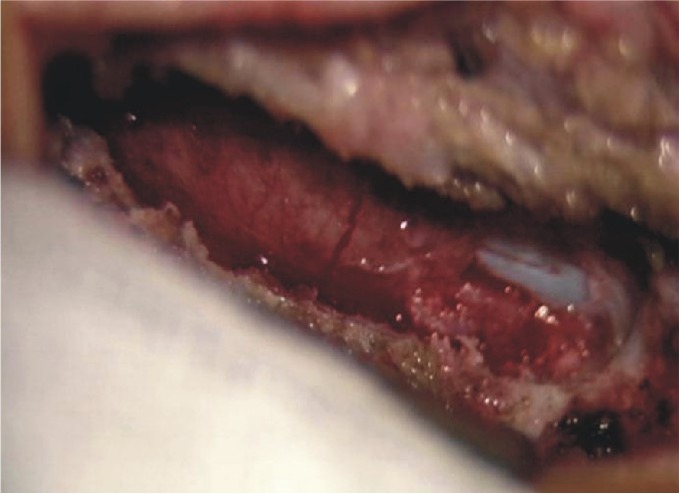
She was not able to walk and sleep due to incapacitating pain. The pain was not relieved by intravenous analgesics. We decided to perform surgical treatment. Under microscopy, left partial laminectomy was done at L2-3 level. The yellow-reddish colored, and flat typed-mass was located between the dura mater and the anterior wall of the L3 lamina (Fig. 2). The mass was soft and easily separated from the dura, lamina, and pedicle. The mass was totally removed.
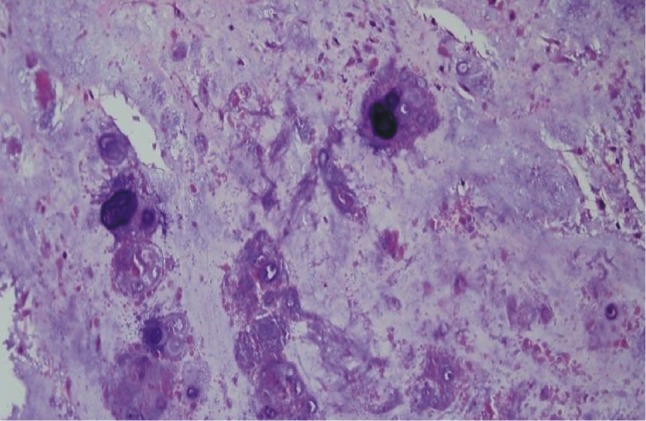
Histopathologic examination revealed that the tumor consisted of chondroma, which had mature hyaline cartilage with nests of benign-appearing cells and calcium deposits in lacunae (Fig. 3).
Postoperatively, the radiating pain was completely relieved. At 3 months after surgery, follow-up MRI showed no remnant mass or recurrence. The patient presented no radiating or back pain anymore.
DISCUSSION
Benign cartilaginous tumors are classified into four histological types: chondroma, osteochondroma, chondroblastoma, and chondromyxoid fibroma2,6,7,9). Chondroma is the most common cartilaginous tumor, and is equivalent to 5% of all bone tumors6). The most common originated sites are long bones of the hands and feet. However, chondromas were sometimes found in the ribs, pelvis, and rarely intracranial bones1,6). Chondromas in the spine are very unusual pathologic entity, accounting for approximately 3% of all chondromas6). Especially, symptomatic chondoromas of the lumbar spine are quite rare and only 16 cases including this case have been reported (Table 1)4,7,12,14).
Chondromas can be subdivided into 2 types according to their site of origin: the medullary cavity (enchondroma) and the surface of periosteum (periosteal chondroma). In this case, the type of the chondroma was periosteal chondromas. The periosteal chondromas can increase in size with broad base, but usually does not infiltrate the adjacent soft tissue. Chondroma can occur at any part of the vertebra including body, pedicle, lamina and spinous process. In our review of literatures, neural arch was the most common affected location in the lumbar spine, accounting on 11 out of 16 cases. Lumbar chondroma could remain asymptomatic or present with back pain, swelling, and sciatica. Although tumors arising from the pedicle or posterior spinal canal could present acute nerve compression, in most of lumbar chondroma, the symptoms slowly develop over several months. However, in current case, the patient presented with acute sciatica aggravated during 1 week without trauma or a past clinical history.
Plain films of lumbar spine show indirect signs of these lesions with smooth erosions of the bone structure, which are radiolucent area or calcification6,7). Computed tomography (CT) demonstrates a soft tissue mass with stippled calcifications and local bone destruction showing isodense or hyperdense3,16). MRI shows a subperiosteal lobulated mass at the bone surface with peripheral rim enhancement on T1WI. Also, MRI revealed hypo- to iso-SI on T1-WI, low-SI on T2WI4,15,17). Furthermore, MRI is important for differential diagnosis because tumor size, pattern, location, and relation of surrounding structures, especially cord compression can be identified6,14).
Nevertheless, differential diagnosis of chondromas from cartilaginous tumors is often difficult based on the radiologic finding alone. Therefore, biopsy is needed for exact diagnosis6). Gross findings of chondroma appear as lobulated and cartilaginous mass with a covering of fibrous tissue from the periosteum8). Histopathologic findings of chondroma are composed of chondrocytes arranged in a pseudolobular fashion and may be associated with ossified regions3).
Surgically total removal is the treatment of choice for lumbar spine chondroma. Recurrence of chondroma is rare and usually related with incomplete removal3,6,7). The important point is that approximately 10% of solitary chondromas undergo malignant progression requiring radiation therapy4,5,11). Malignant progression is related with a component of syndrome, Ollier's syndrome and Maffucci's syndrome4).
CONCLUSION
We report a rare case of chondroma in the lumbar spine presenting acute sciatica in a 47-year-old woman. Although lumbar chondroma is unusual and slowly growing, it should be considered in the differential diagnosis of extradural mass in patients with acute sciatica. In lumbar spine chondroma, total surgical resection is the treatment of choice for immediate relief of sciatica and avoiding a recurrence.










")













