






INTRODUCTION
Lumbar posterior apophyseal ring fracture (PARF) is an uncommon disorder first described by Meyenburg in 1946 [1], that occurs predominantly in adolescents, especially young athletes [2,3]. The lesion is characterized by the separation of the bony fragments at the posterior rim of the lumbar vertebral endplate, projecting into the spinal canal [2,4,5]. In most cases, PARF is accompanied by lumbar disc herniation (LDH), resulting in low back pain and nerve compression symptoms [4,6]. Due to the persistence of spinal canal compression, some authors support early surgical intervention after simple conservative treatment [4,7,8]. Over the last 3 decades, the clinical outcome of conventional open surgery for PARF combined with LDH has been recognized [9-11]. Meanwhile, some authors have reported a series of challenges encountered during open surgery, such as decisions regarding intervertebral disc removal without removal of bone fragments that have not caused symptoms, the need for fusion, and the avoidance of dura injury [9,11,12].
Recently, minimally invasive surgery has become popular and has advantages over conventional open surgery such as the preservation of the natural anatomy to the maximum extent and reduction of postoperative complications [13]. Transforminal endoscopic lumbar discectomy (TELD) is an ultra-minimally invasive surgical technique, and its indications have been extended from purely inclusive disc herniation, to the removal of various types of LDH and prolapse, as well as in the expansion of foramina [14]. This emerging minimally invasive surgical technique in the treatment of PARF combined with LDH encounters some of the same challenges as open surgery in these patients [6,7]. Therefore, there is a learning curve for inexperienced surgeons. However, there is scant literature on the clinical outcomes and management experience of performing minimally invasive treatment for PARF patients.
The aim of this study was to compare the treatment and outcomes in patients with PARF combined with LDH and those with LDH without PARF. In a series of 1,324 consecutive LDHs seen in our department, 48 patients underwent TELD for PARF accompanied by LDH. The control group was comprised of 50 patients diagnosed with LDH without PARF at the same facility.
MATERIALS AND METHODS
1. Patient Population
The study was approved by the Ethics Committee of Beijing Chaoyang Hospital (registration number: 2021-KE-25) and the research was performed in accordance with the guidelines of the Declaration of Helsinki. Through medical records, we identified 48 patients with PARF associated with LDH who underwent TELD in our department of orthopedics between January 2013 and December 2019. These patients were considered as the PARF group. Between January and June 2015, we treated 50 consecutive LDH patients without PARF; these were considered as the control group. Before surgery, conservative treatment was recommended, including bed rest and cobamamide injections. All patients were older than 18 years, and patients with a history of spondylolysis, spinal infection, severe spinal stenosis, tumors, or systemic diseases that affect the bone or joint were excluded. Patients with PARF occurring simultaneously in the upper and lower endplates or multiple spinal segments were excluded.
2. Operative Technique
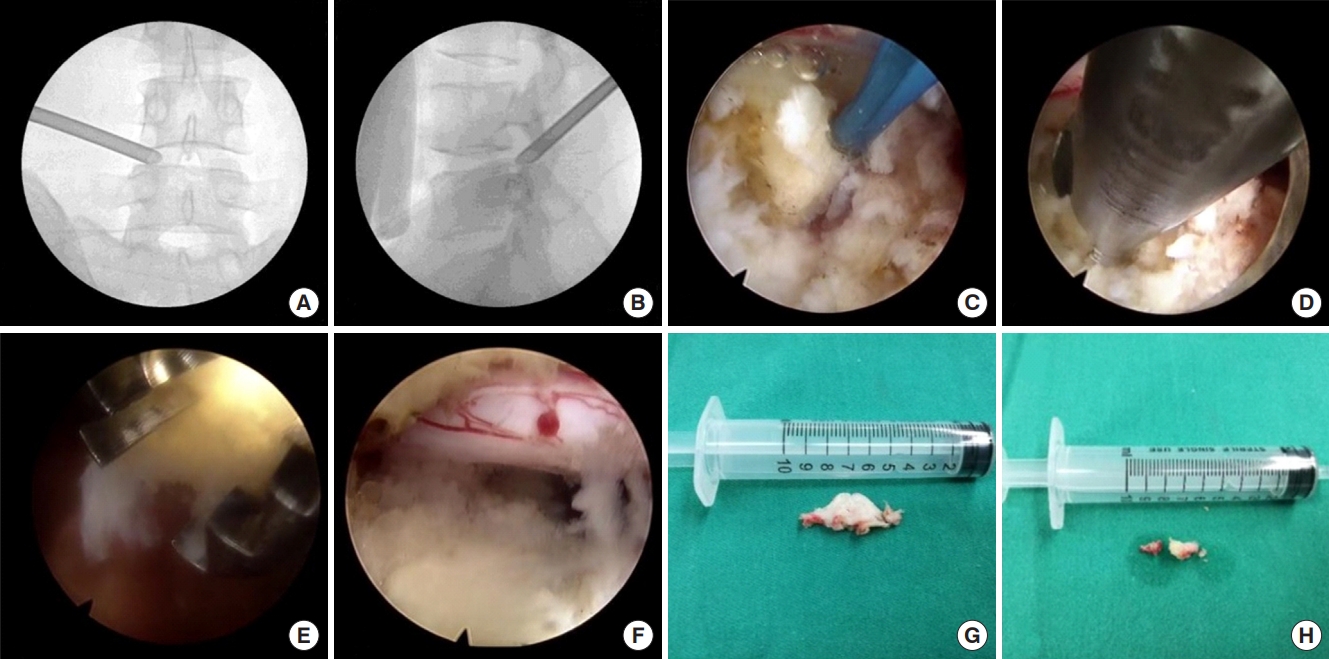
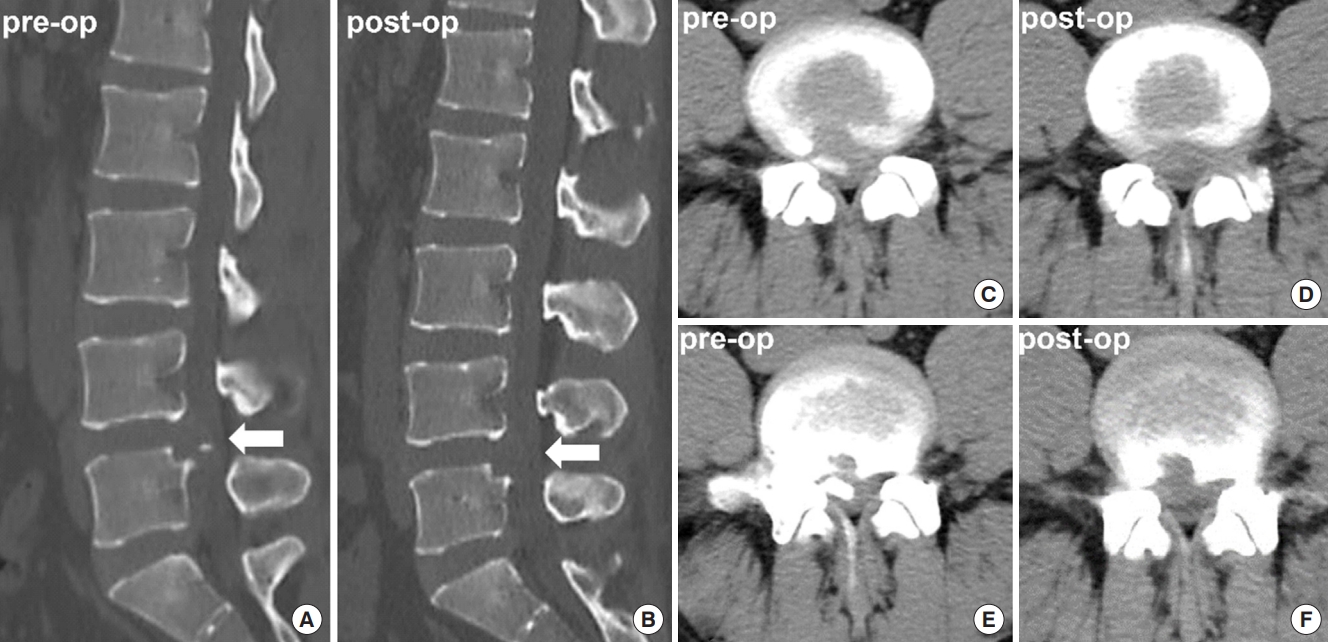
For the TELD procedure, the patient was placed prone, and the entry point of the assumed approach was 12 to 14 cm lateral to the midline of the spine at the affected intervertebral level. A guidewire was docked onto the targeted segment. The paravertebral muscles were dissected using serial cannulated dilators, 5-g/L lidocaine was used for infiltration and anesthesia around the facet, and a tubular retractor with an outer diameter of 7.5 mm was placed (Fig. 1A, B). Next, if the intervertebral foramen did not provide adequate surgical access to the spinal canal, burrs were used to further enlarge the opening. Under direct vision, decompression was performed using constant irrigation. The herniated disc and bone fragments were completely resected using a rongeur (Fig. 1C–H), and the mobile fragment around the nerve root was removed using a curette. If necessary, the bone could be crushed using a rongeur and then removed. Bipolar electrocoagulation was applied to promote hemostasis during operation. In addition, hemostatic gauze and gelatin sponge can be used to stanch the bleeding by compressing oozing bony surfaces. A wound drain can be placed as necessary to prevent postoperative hematoma. After irrigation and hemostasis, the surgical wounds were sutured in an anatomical order. Representative cases are presented in Fig. 2.
3. Come Assessment
The following general parameters were recorded for both patient groups: sex, age, levels of disc herniation, symptoms, history of trauma, preoperative neurological deficit, and duration of symptoms. We reviewed the medical records for operation duration, first ambulation time, complications, and the rate of recurrent LDH. Clinical outcomes were defined as excellent, good, fair, and poor according to the modified MacNab criteria [15]. Statistical evaluation of clinical outcomes at the last follow-up was performed.
4. Data Analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA). Data are shown as mean±standard deviation. Paired-samples t-tests were used for continuous variables, and the chi-square test and Fisher exact test were used for categorical variables. Statistical significance was set at p<0.05.
RESULTS
The patient characteristics in the PARF group are summarized in Table 1. A total of 48 adult patients diagnosed with PARF associated with LDH who underwent TELD were included in this study (38 [79.2%] men, 10 [20.8%] women). Mean duration of the final postoperative follow-up was 5.1 years (range, 2.2–8.6 years). The average age was 38.7 years (range, 18–57 years). There was a clear history of trauma in 7 patients (14.6%) attributed to weight lifting and falls. It should be noted that trauma that is not directly related to PARF, and sedentary fatigue is not included in the statistics.
The average duration of symptoms was 12.7 months (range, 0.5–38 months). The predominant symptom was leg pain in 42 patients (87.5%) and lower back pain in 6 patients (12.5%). There were 39 (81.3%) PARF patients without normal preoperative neurological examinations, 8 patients (16.7%) showed decreased muscle strength of the lower limbs and shallow hypoesthesia, 4 patients (8.3%) showed asymmetric tendon reflexes, and 1 patient (2.1%) had cauda equina syndrome.
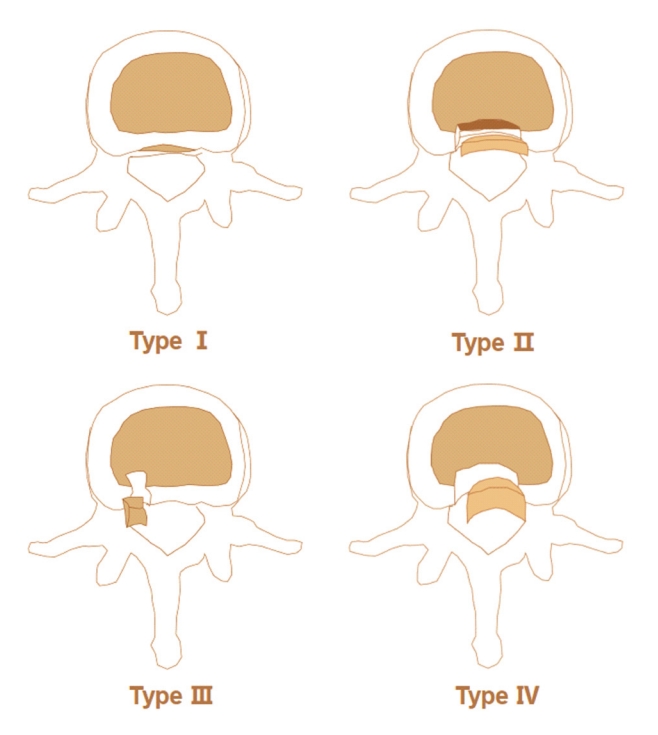
Computed tomography (CT) images were reviewed to classify PARF into 4 types according to the Takata’ classification (Fig. 3) [16]. The most common category was type II (43.8%), followed by type I (33.3%), and type III (22.9%) (Table 2). Our department has not treated a patient with type IV PARF. The most frequently involved site of PARF disease was the lower endplate of the L5 vertebral body (39.6%). All apophyseal ring fractures were at the same level as disc herniations. Forty-two cases (87.5%) had herniated discs located on the lateral side, and 6 cases (12.5%) had a central disc herniation. The number of small PARF was 26 (54.2%) and the number of large PARF was 22 (45.8%) (small or large, defined by 50% width of spinal canal [4]).
Clinical outcomes are summarized in Table 3. Thirty-three patients (68.8%) had excellent results, 8 (16.7%) had good results, 6 (12.5%) had fair results, and 1 (2.1%) demonstrated poor results. Postoperative CT scans were performed in all 48 PARF patients, and the results showed that intact bone fragments were removed in 45 cases (93.8%). In the remaining 3 cases (6.2%), decompression around the nerve root was adequate, although complete bone fragments were not removed. The mean operation time in the PARF group was 105.4 minutes (range, 75–135 minutes), which was longer than the control group (83.9 minutes; range, 65–105 minutes) (p<0.05). In 2 patients (4.2%), we experienced surgical instrument rupture during the operation, but there were no residual instruments. Three patients (6.3%) experienced dural tears during surgery, and one of them required intraoperative repair due to cerebrospinal fluid leakage. Recurrence developed in 2 patients (4.2%); both required reoperation at the same level (at 5 months and 2 years, respectively).
DISCUSSION
PARF is an uncommon disorder that is usually accompanied by LDH. Conventional open surgery was frequently recommended for PARF over the past 3 decades, with excellent and good rates of 85% to 97% [9,11]. However, open surgery can cause greater trauma and loss of lumbar mobility [11,17], which is not conducive to the young population in which PARF is most common. TELD is an ultra-minimally invasive surgical technique. We reviewed our experience of the last 7 years of using TELD for the treatment of PARF, and found a good or excellent outcome in 85.4% of 48 patients. In addition, we found an average first ambulation time of 18.6 hours, and 35 patients (72.9%) returned to work within 2 months postoperatively. Although minimally invasive surgery has proven to be more advantageous than conventional open surgery in terms of maximal preservation of natural anatomy, these advancements require a longer learning curve for inexperienced surgeons [13]. There are several issues of concern, including indications, decisions regarding apophyseal fragment removal, surgical approach, and complications.
Surgical indications for PARF remain controversial. Most authors [6,11,18] support the necessity for surgical intervention for PARF with neurological deficits. Most of the controversy concerns whether PARF without neurological deficits (only low back pain and/or leg pain) requires surgery [4,19]. Asazuma et al. [12] and Bae et al. [20] found that conservative treatment is ineffective in many cases with the evolution of chronic low back pain, and recommended surgical treatment. However, Krishnan et al. [21] reported that among 19 patients without neurological deficits, 12 responded well to conservative treatment, and only 7 cases required surgical treatment. Chang et al. [4] reported that 3 of 12 patients without neurological deficits had poor outcomes during conservative treatment. We believe that the above literature highlights the need for surgery in the background of the widespread popularity of open surgery in past years. In such scenarios, some authors may have preferred conservative treatment in order to avoid the shortcomings of open surgery such as large trauma to the anatomy, slow recovery, and loss of lumbar mobility. The authors of the present study suggest that the bone fragment clearly participates in pathogenic factors, and the rapid recovery seen in minimally invasive surgery can be partially attributed to the prevention of recurring symptoms and prolonged chronic pain that may have resulted if pathogenic factors were not removed.
Of concern is whether minimally invasive TELD can be used to remove large bone fragments, and whether the size of bone fragments is a factor in choosing minimally invasive or open surgery. In our study, 22 cases (54.2%) of large PARF were included, and the excellent and good rates were not significantly different from those with small PARF. Moreover, Matsumoto et al. [22] reported that microendoscopic discectomy, another minimally invasive technique, can also complete the resection of a large PARF. There are 2 reasons why minimally invasive surgery can remove a large PARF: (1) in minimally invasive surgical procedures, large bone fragments are usually gradually removed by rongeurs and blue forceps bit by bit and not necessarily to preserve the integrity of the bone fragment; (2) a report of CT axial scans of patients with PARF showed that the bones are usually in strips, and the left and right diameters are significantly larger than the anterior and posterior diameters [20]. In view of this situation, if the bone block is found to be unstable during the operation, the block can be removed along the direction of the tubular retractor. Therefore, the authors believe that the size of PARF should not be used as a factor in selecting the appropriate surgical procedure. However, multi-segment PARF and severe spinal stenosis are indications for open surgery [19,20].
A related issue is the consideration of complete removal of the bone fragment [6,11,20]. In our study, partial PARF resection was performed in 13 patients (27.1%) with an excellent and good rate of 92.3%, and total resection was performed in 35 patients (72.9%), with an excellent and good rate of 94.2%. In addition, in a randomized controlled study with a mean follow-up of 4.3 years, Shirado et al. [9] found that bone fragment resection did not affect clinical outcomes. However, most authors advocate that bone fragments should be completely removed, and the clinical results of several studies were satisfactory [12,21-23]. The authors of the present study believe that the source of this controversy is: (1) some bone fragments are not the cause of the disease; (2) some bone fragments did not worsen clinical outcomes at long-term follow-up; and (3) some bone fragments are also involved in maintaining spinal stability. The authors recommend that the bone fragments that are clearly involved in the disease should be removed, and whether the bone fragments are less likely to cause disease should be based on the results of comprehensive consideration, including the surgical difficulty of bone removal, surgical risk, spine stability, and physical condition. Although the removal of bone fragments is controversial, most authors recommend removal of the disc accompanied by bone fragment [11,12,22,23]. However, it is worth noting that PARF occurs mainly in adolescents, and discectomy should be considered with caution [11,24].
Full-endoscopic lumbar discectomy treatment of PARF can usually be divided into 2 types: the transforaminal approach and the interlaminar approach [6,22]. In our study, all 48 patients received the transforaminal approach and achieved satisfactory clinical outcomes with an excellent and good rate of 85.4%. However, Matsumoto et al. [22] and Zheng et al. [6] also achieved satisfactory clinical results using the interlaminar approach for the treatment of PARF. The authors of the current study believe that the transforaminal approach has more advantages in the concept of targeted puncture, the means of enlarging the intervertebral foramen, and the specialized surgical instruments which cause less iatrogenic damage to the nerve root. However, a laminar approach is recommended for patients for whom the transforaminal approach would be obstructed by the high iliac crest, hypertrophic transverse process, or fusion of the L5 transverse process and iliac crest [9]. In addition, translaminar surgery may be recommended in cases with large bone fragments. This is mainly because it is more convenient to resect the large bone fragment from top to bottom (interlaminar approach) than from bottom to top (transforaminal approach) during the operation. It is worth noting that, unlike open surgery, fusion is not recommended routinely in minimally invasive surgery for PARF [25,26]. Talha et al. [25] and Baba et al. [26] suggested that if extensive bilateral laminectomy is performed, fusion may be necessary to avoid secondary instability. However, the minimally invasive approach for PARF does not rupture the lamina or damage the paraspinal muscles that maintain the stability of the spine [27].
The main complications of minimally invasive treatment of PARF include dural tear nerve root injury, surgical instrument rupture, postoperative infection, and recurrence [6,22,28]. In our study, 3 patients (6.3%) developed dural tear, 2 patients (4.2%) developed recurrent LDH, and surgical instrument rupture occurred in 2 patients (4.2%). In studies reporting the results of open surgery for PARF [10,11,20], dural tear occurred in 1.2% to 7.4% of patients, and recurrent LDH occurred in 4.6% to 12.7% of patients. The complication rates of these reports and our report are similar. However, in minimally invasive treatment of PARF, surgical instrument rupture and dural tears are more common than in the treatment of pure LDH. This is because the fine micro rongeurs are easy to rupture or even remain when the hard bones are clamped roughly. Therefore, it is important to try the hardness of the bone block during the first clamp. If the texture is found to be hard, then you need to bite off the bone block bit by bit patiently from the surrounding area. In addition, the pathological changes of PARF are complex and slow, the spinal dura mater and nerves are compressed for a long time, and local inflammation causes scar adhesion [11], which may be the main reason why PARF is more common than dural tears in pure LDH. Moreover, we recommend removing the herniated disc first, and then “biting off” the bone that compresses the nerve root. After the herniated disc is removed, the nerve tension is reduced, which can avoid the complications of nerve injury caused by excessive nerve traction. Thus, the separation and removal of bone fragments, which is a key step in the procedure, requires patience and care.
The current study had several limitations. First, although PARF is divided into 4 types, there is no authoritative region division based on the prominent position of the bone block, which is a very important consideration for the choice of surgical approach. Investigation of this concept requires the support of multicenter, large sample, and long-term follow-up outcome studies. Second, patients in our center with PARF at multiple levels underwent open surgery and were not included in this study; their treatment plan needs to be supported by further study outcomes. Finally, further studies are necessary to better understand the pathoanatomy and pathophysiology of this disease.
CONCLUSION
In summary, our findings show that TELD is a safe and effective minimally invasive approach for the treatment of PARF with LDH. Minimally invasive surgery may require a longer learning curve for inexperienced surgeons. The authors hope that this study will provide valuable insights into minimally invasive techniques for the treatment of PARF.










")













