






INTRODUCTION
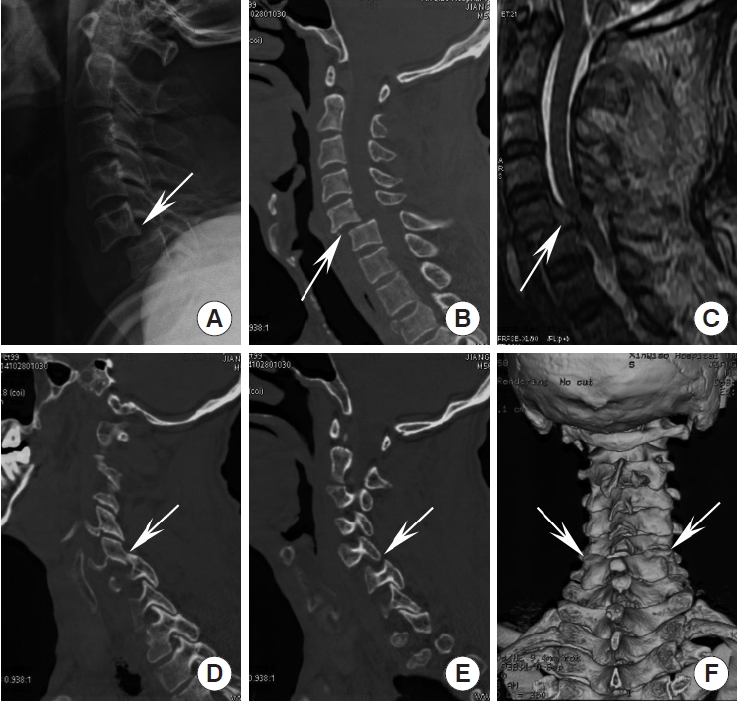
Lower cervical facet dislocation is a common spinal trauma caused by flexion-distraction force that usually results in damage to the 3-column structure, as well as vertebral dislocation, facet locking, and intervertebral disc destruction (Fig. 1). The treatment of lower cervical facet dislocation is generally recognized as reduction, decompression, fixation, and fusion. Early reduction can reduce the compression of the spinal cord, which is particularly important for patients with incomplete spinal cord injury. Since Walton et al. [1] first reported closed reduction by manipulation of cervical spine deformity caused by facet dislocation in 1893, great advancements have been made in reduction techniques, especially in recent years. In the present study, we review all reduction techniques, including traditional, popular, and novel techniques. In general, the reduction techniques are categorized into 4 main types: closed reduction, anterior alone, posterior alone, and combined approach techniques.
CLOSE REDUCTION TECHNIQUES
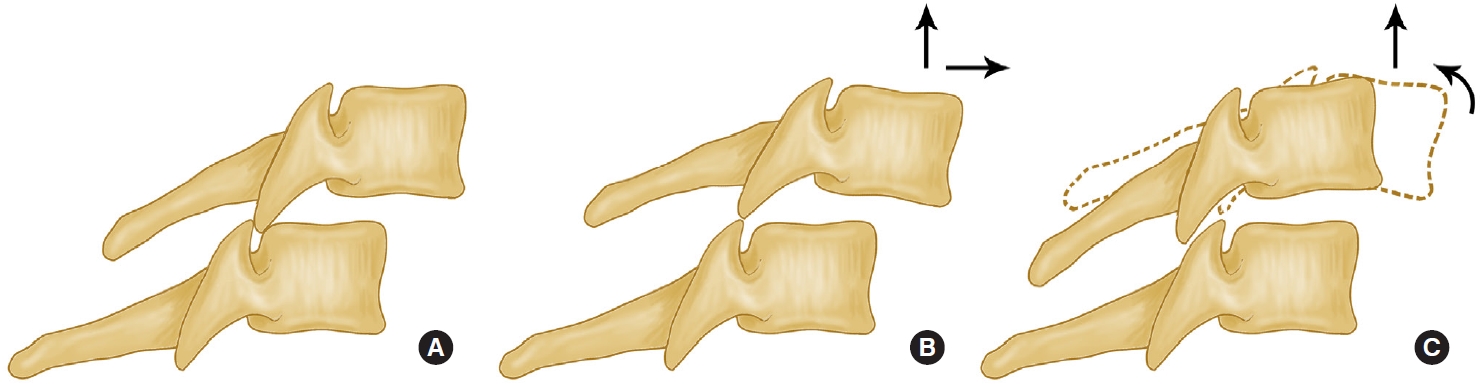
Close reduction was the initial technique for lower cervical facet dislocation. After Walton et al. [1] first described closed reduction by manipulation of cervical facet dislocation in 1893, Crutchfield et al. [2] introduced tongs for in-line traction-reduction in 1933. Thereafter, closed reduction of the cervical spine using head traction has been used for many years and reported as an effective treatment for many cervical facet dislocations [3-25]. Although the technique of manipulation varies from surgeon to surgeon, the basic procedure is a gradually traction, followed by anterior rotation and lateral flexion away from the side of the dislocated facets. while the locked facets have been disengaged, rotation is carried out in the opposite direction. As soon as a click is heard or felt, the neck is extended (Fig. 2).
Although the principle of closed reduction is basically the same, there are also some differences and controversies in various literature views. Firstly, the weights required to be traction reported in the previous literature were different [26-28]. Reindl et al. [27] reported that all patients were treated with Gardner-Wells traction, starting with 5 kg+2.5 kg/level of injury below C1. This was followed by addition of 2.5 kg every 30 minutes until reduction was achieved, to a maximum of 50% estimated body weight for 1 hour. In the cases report of Tumial├Īn et al. [24], an initial traction weight of 9.1 kg was applied, followed by an increase of 4.5 kg per hour. Once 27.2 kg was reached, the lateral radiograph was suggestive of reduction. Miao et al. [25] retrospectively analyzed 40 patients. The initial traction weight was 5 kg, and if the weight reached 15 kg, closed reduction could be completed in most patients (38 cases, 95%). This difference may depend on the state of the articular process after facet dislocation. If the facets are fractured, the reduction may occur with lower weights, and good alignment will be achieved easily. Otherwise, if the facets are locked, too many weights are necessary, a reduction may be severe. Moreover, if the dislocation is delayed, closed reduction is almost impossible.
Secondly, there is still some controversy as to whether or not anesthesia is performed during traction-reduction. The observations of Evans [3] and Kleyn [7] popularized reduction under anesthesia, although other authors condemned the procedure as potentially dangerous compared with craniocervical tractionreduction. In 1994, a cohort study performed by Lee et al. [29] found a higher rate of success and a lower complication rate with traction-reduction as opposed to manipulation under anesthesia. In 1999, a prospective observational study by Vaccaro et al. [21] assessed the safety of awake closed reduction maneuvers in 11 patients with cervical spine dislocations. The results showed that none of the patients in their study suffered from neurological worsening during or after closed reduction. Suitably, Vaccaro et al. [21] stated in the conclusion of the article that the implications related to the ŌĆ£neurologic safety of awake closed reduction traction reduction remains unclear.ŌĆØ However, there were also many authors who believed that manipulation under anesthesia was still a frequently practiced technique, usually used after failure of traction-reduction but occasionally used as a primary means of achieving reduction [11,30,31].
Thirdly, the need for magnetic resonance imaging (MRI) before reduction is a matter of debate. Some investigators believed that disc disruption in association with facet fracture-dislocation increases the risk of spinal cord injury by disc material after reduction [2,8,29,32]. Rizzolo et al. [33] found evidence of disc disruption/herniation in 42% of patients studied with prereduction MRI. Darsaut et al. [34] recommended MRI-guided reduction due to their observation of an incidence of 88% cervical disc disruption before closed reduction. Hart et al. [35] also believed that prereduction MRI was crucial, basing his argument on the supreme cost incurred if the diagnosis was missed even rarely. So, they recommend the use of prereduction MRI to assess for ventral cord compromise caused by traumatic disc disruption. On the other hand, some authors have found no relationship between findings on prereduction MRI, neurological outcome, or findings on postreduction MRI [5]. et al. [21] based his opinion that MRI was unnecessary in many cases on extensive clinical experience and prospective clinical data. A basic animal research has demonstrated that a relatively brief window of 1 to 3 hours is available, after which injury to the spinal cord caused by mechanical compression may become irreversible [36]. The use of prereduction MRI may delay reduction of the spinal deformity and therefore may delay decompression of the compromised spinal cord. Moreover, prereduction MRI assessment requires the transport of a patient with a highly unstable cervical spine fracture to the MRI suite. Many laboratories work also suggested that early reduction of fracture-dislocation injuries may improve neurological outcome [3,11,32,37].
In previous reports, the success rate of closed reduction ranged from 30% to 100% [9,18,20,38] (Table 1). Those who failed closed traction reduction should perform open reduction as soon as possible. Many papers reported that closed reduction attempts could not be successful in all cases [39]. Some surgeons suggested that closed reduction was only suitable for conscious and cooperative patients, and for severely injured uncooperative patients, rapid open surgical reduction should be selected [40,41]. Besides, even after a closed reduction, open surgery with stabilization of the dislocated level is necessary. Since closed reduction requires close neurologic monitoring, imaging to monitor progress is not always feasible [42]. Some surgeons prefer to make an open reduction and stabilization surgery at the same sitting for those reasons. Lambiris et al. [43] believed that all patients with lower cervical facet dislocations had cervical spine instability due to soft tissue injury of the dislocated segment. Open surgery should be used to quickly stabilize the cervical spine, so that patients could exercise as soon as possible, which was beneficial to recovery. The cervical spine function could also avoid long-term external fixation and related complications. Dvorak et al. [44] conducted a controlled study of 90 patients and concluded that patients with open surgery had a better prognosis than patients with nonsurgical treatment. It was recommended that all patients should undergo open surgery after cranial traction. In summary, there is still a controversy about performing a closed reduction compared with open surgical reduction and fixation [39].
OPEN SURGICAL REDUCTION TECHNIQUES
The surgical treatment of patients with lower cervical facet dislocation is indicated to improve neurologic deficit, to restore spinal mechanics through correction of a deformity, to stabilize unstable lesions, and to facilitate the patientŌĆÖs comfort [43,45]. There are many ways of surgical reduction, including anterior approach, posterior approach, and combined anterior-posterior approach. The choice of surgical way depends on many factors, including the patientŌĆÖs neurological status, whether it is combined with traumatic disc herniation, the success of closed reduction, unilateral or bilateral facet dislocation, whether there is a vertebral fracture or accessory fracture, and the surgeonŌĆÖs experience and habits [46].
1. Anterior-Only Approach Techniques
Anterior-only approach surgery is mainly suitable for patients with structural injuries on the ventral side of the spinal cord, especially for the patients with traumatic disc herniation. Anterior-alone approach is surgically less traumatic owing to its blunt interplane dissections. Infection rate is lower compared with the posterior approach (0.1% to 1.6% vs. 16%) [47]. Direct access to the injured intervertebral disc enables decompression via discectomy.
Anterior stand-alone interbody bone grafting and fusion of lower cervical spine fracture dislocation was recognized and widespread following reports by Bailey and Badgley (1960), Cloward (1961), and Verbiest (1962). It was further refined by Bohler (1964), Orozco (1970), Tschern (1971), Senegal (1971), and Gassman and Seligson (1983) with the introduction of plate and screws to tackle earlier complications related to secondary deformity and graft extrusion [48]. In 1973, Cloward [49] reported a new surgical technique and instrument they called ŌĆ£cervical dislocation reducer,ŌĆØ which treated a patient with an unusual cervical dislocation successfully. de Oliveira [50] introduced that 12 patients with locked facets of lower cervical spine were surgically treated through an anterior approach using interbody disc spreaders in 1979. Since then, due to the unique advantages of anterior-only surgery, it has been widely popular, and the techniques and instruments have undergone continuous improvement [51-53].
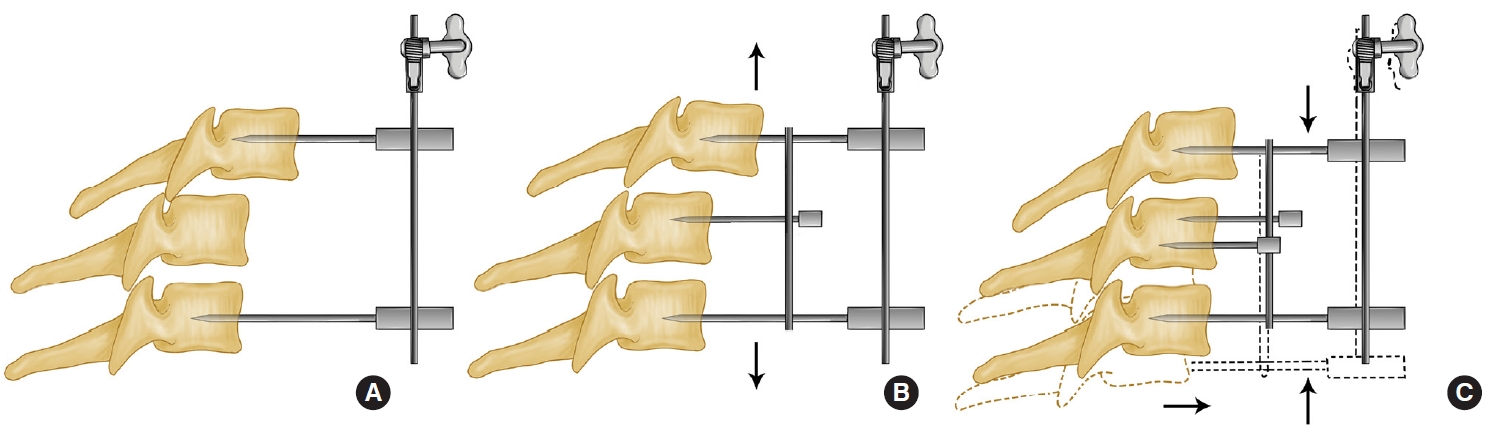
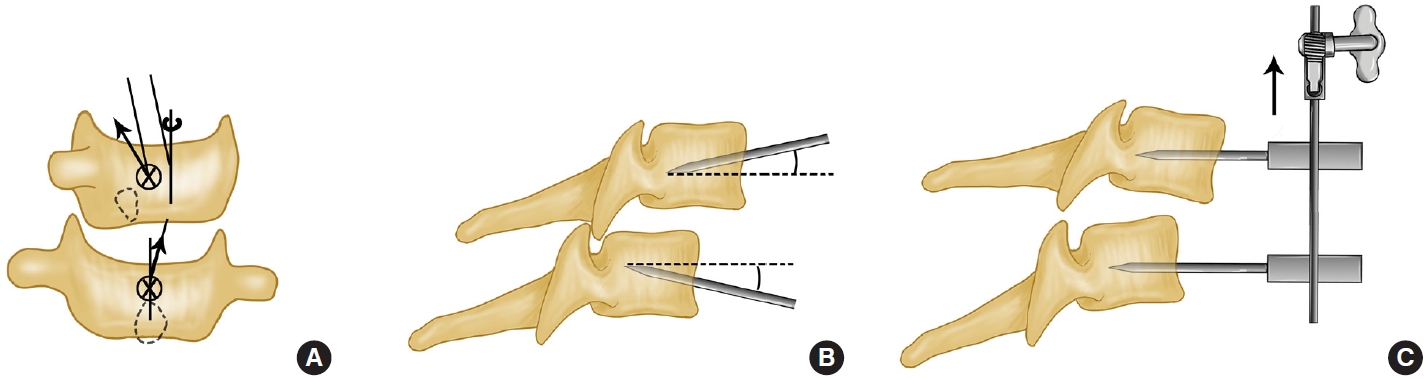
In 2000, Ordonez et al. [54] reviewed the previous experience and introduced the reduction techniques in detail with the anterior surgical approach in 10 patients with either unilateral or bilateral cervical facet dislocation. After a standard anterior approach discectomy to the cervical spine, vertebral body posts (Caspar or equivalent devices) were placed at approximately a 10┬░ to 20┬░ divergent angle with respect to each other. Angling the vertebral body posts provides for the application of a bending moment when distraction was applied. While the locked facets were disengaged, dorsally directed pressure to the rostral vertebral body into normal alignment could be applied using manual pressure or a curette (or similar device) (Fig. 3).
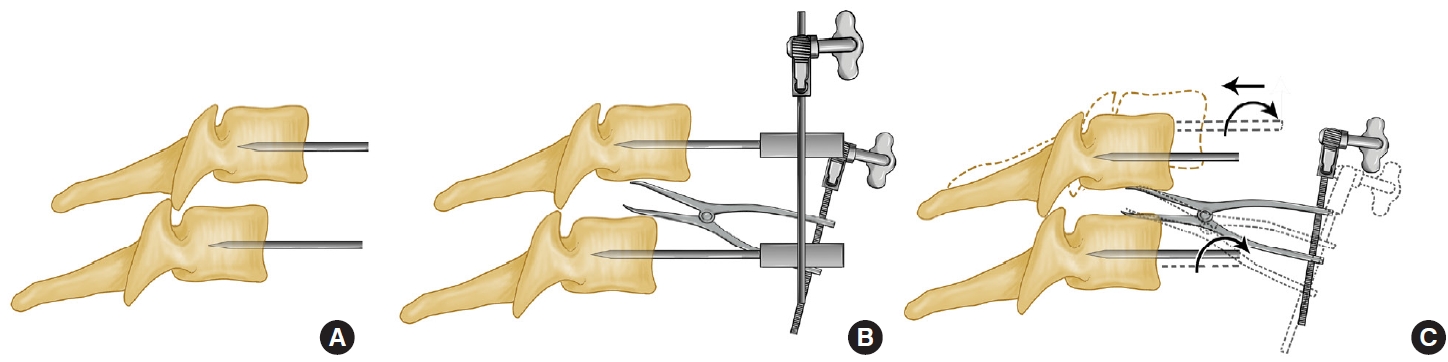
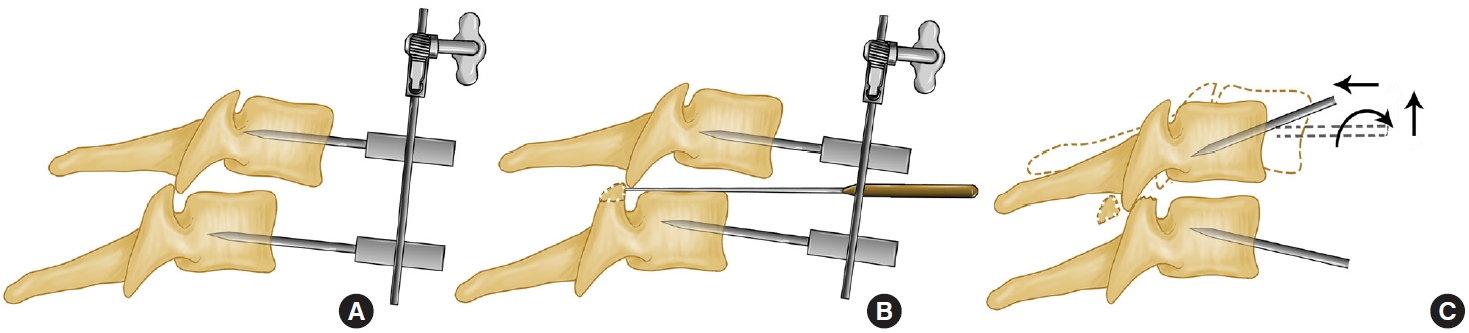
This technique was improved and supplemented in reports by Reindl et al. [27] in 2006 and Ren et al. [55] in 2020. There was still application of the Caspar retractor system with pins at the level above and below the subluxation or dislocated segments. The pins were placed in a convergent manner to apply a slight amount of kyphosis during the distraction maneuver. If this was not effective, a laminar spreader (Reindl) or a periosteal detacher (Ren) was inserted at the affected disc space. Distraction and cephalad rotation of the instrument were then used to unlock the dislocated facets (Fig. 4).
In 2014, Du et al. [56] reported that 17 patients monitored by spinal cord evoked potential were successfully reduced using a trial-model device as a lever. With spinal cord evoked potential monitoring, standard transverse incision was performed. After removal of disc and opening the posterior longitudinal ligament, anterior decompression of spinal cord was completed. Skull traction was maintained utile the inferior articular process of dislocated vertebrae was just right on top of the superior process of inferior vertebrae. Then they poked the inferior vertebrae to unlock the facet dislocation (Fig. 5).
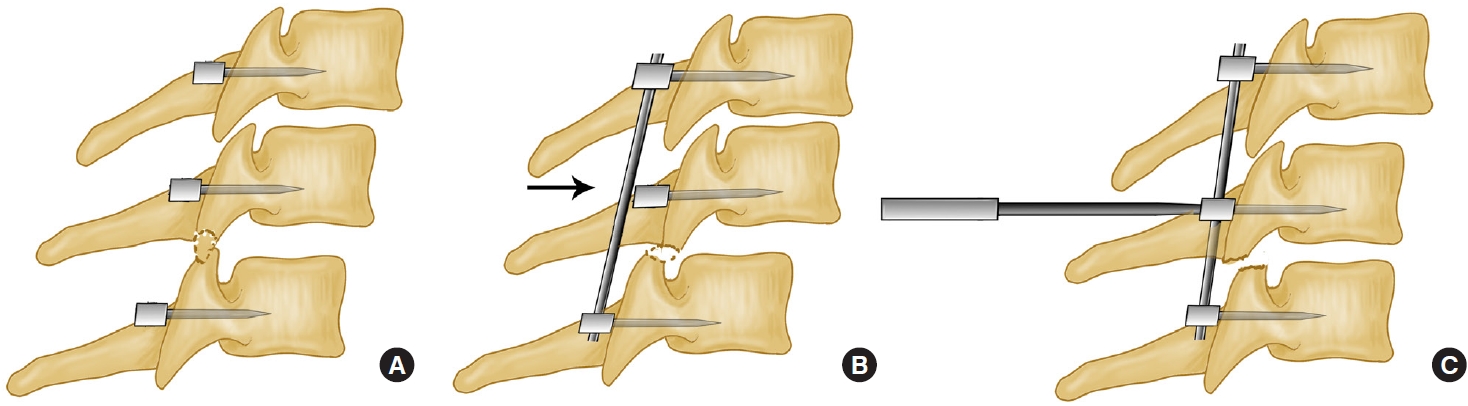
Unfortunately, for some patients with delayed treatment or osteoporosis, the distraction force of conventional techniques may not be able to completely disengage the locked facets. In 2017, Zhang [57] reported the successful reduction of 4 patients with unilateral facet dislocation using the anterior pedicle distraction reduction technique who failed to use the vertebral distractor reduction technique. After anterior discectomy, a pedicle distractor (anterior screw tapper) was implanted from the anterior approach along the axis of the pedicle under fluoroscopy monitoring. The trial model used as a fulcrum was placed into the intervertebral, and the distractor could directly act the force on the locked facet. Then pressed down the spreader to pry and disengage the facet. When the inferior articular process of dislocated vertebrae was just right on top of the superior process of inferior vertebrae, the upper vertebrae was pushed in a caudad direction to achieve reduction (Fig. 6).
In 2017, Li et al. [58] believed that the conventional anterior approach techniques still had many disadvantages. Attention should be paid to intervertebral instrument insertion depth and the prevention of secondary spinal cord injury caused by instantaneous springing at the time of reduction. They reported a new anterior cervical distraction and screw elevating-pulling reduction technique. The 1st vertebral body superior of the involved segment and the 2nd vertebral body inferior thereto was drilled. After Caspar pins were driven into the drilled holes, Caspar vertebral body retractor was installed and used for longitudinal distraction until a certain tension of surrounding soft tissues was reached. An anterior cervical titanium plate with a length equal to the distance of distraction by the retractor was placed between 2 Caspar pins. Then a half-thread cancellous bone screw of appropriate size was driven into the middle of the plate to pull the dislocated vertebrae until it was pressed against the titanium plate (Fig. 7).
Moreover, Kanna et al. [47] also believed that the simultaneous application of traction and reduction maneuver using the same instrument (Caspar distracter or interbody spreader) did not allow un-locking of the facets. Repeated reduction attempts could be dangerous to the neural tissue and surrounding vascular structures. Hence, they introduced a modified anterior reduction technique used separate instruments in 2017, one for maneuvering the vertebral body and another for interbody distraction, to consecutively treat cervical facet dislocations. After identifying the subluxate segment, Caspar pins were placed on adjacent vertebral bodies parallel to the vertebral endplates in the craniocaudal plane and gently distracted under fluoroscopy monitoring. In the medio-lateral plane, it was essential to place the pins perpendicular to the plane of displacement in uni-facetal subluxation. Anterior cervical discectomy was performed ensuring complete decompression beyond the posterior longitudinal ligament and till the uncovertebral joints on either side. At this stage, the Caspar pin distracters were used for distraction, and an interbody spreader was placed between the vertebral bodies to sustain the distraction. And then the Caspar distracter was now removed leaving the Caspar pins in the vertebral body. The interbody spreader acted only as the distracter while the Caspar pins were used as ŌĆ£joy sticks.ŌĆØ The pins were moved to provide a transverse rotation or flexion-extension moment, depending on the side of facet subluxation (Fig. 8).
Even if the reduction techniques all above failed, Liu and Zhang [59,60] also proposed a novel anterior-only surgical procedure including kyphotic paramedian distraction with Caspar pins and anterior facetectomy in 2019. The successful rate of reduction was reported to be 100%. Kyphotic Paramedian Distraction with Caspar Pins: The level of the injured cervical spine was exposed through a standard Smith-Robinson approach. Two Caspar pins were placed at approximately a 10┬░ to 20┬░ with respect to each other in the sagittal plane. But the entry point and direction of the upper pin should be biased toward the dislocation side to provide greater distraction forces on the dislocated joint. Thus, the distraction was presented in a kyphotic paramedian manner, which mimicked segmental flexion to help facet subluxation (Fig. 9). This technique could reduce most lower cervical facet dislocations. Anterior facetectomy: This procedure was applicated after the failure of the kyphotic paramedian distraction technique. Anteromedial foraminotomy was performed by resection of posterior foraminal portion of the uncovertebral joint. After the nerve root was retracted in a cephalad direction in the neuroforamina, the edge of the dislocated superior facet was broken to achieve reduction. The Caspar retractor was pushed in a posterior direction to achieve posterior translation of upper segment and the broken lower segment (a part of the superior facet) (Fig. 10).
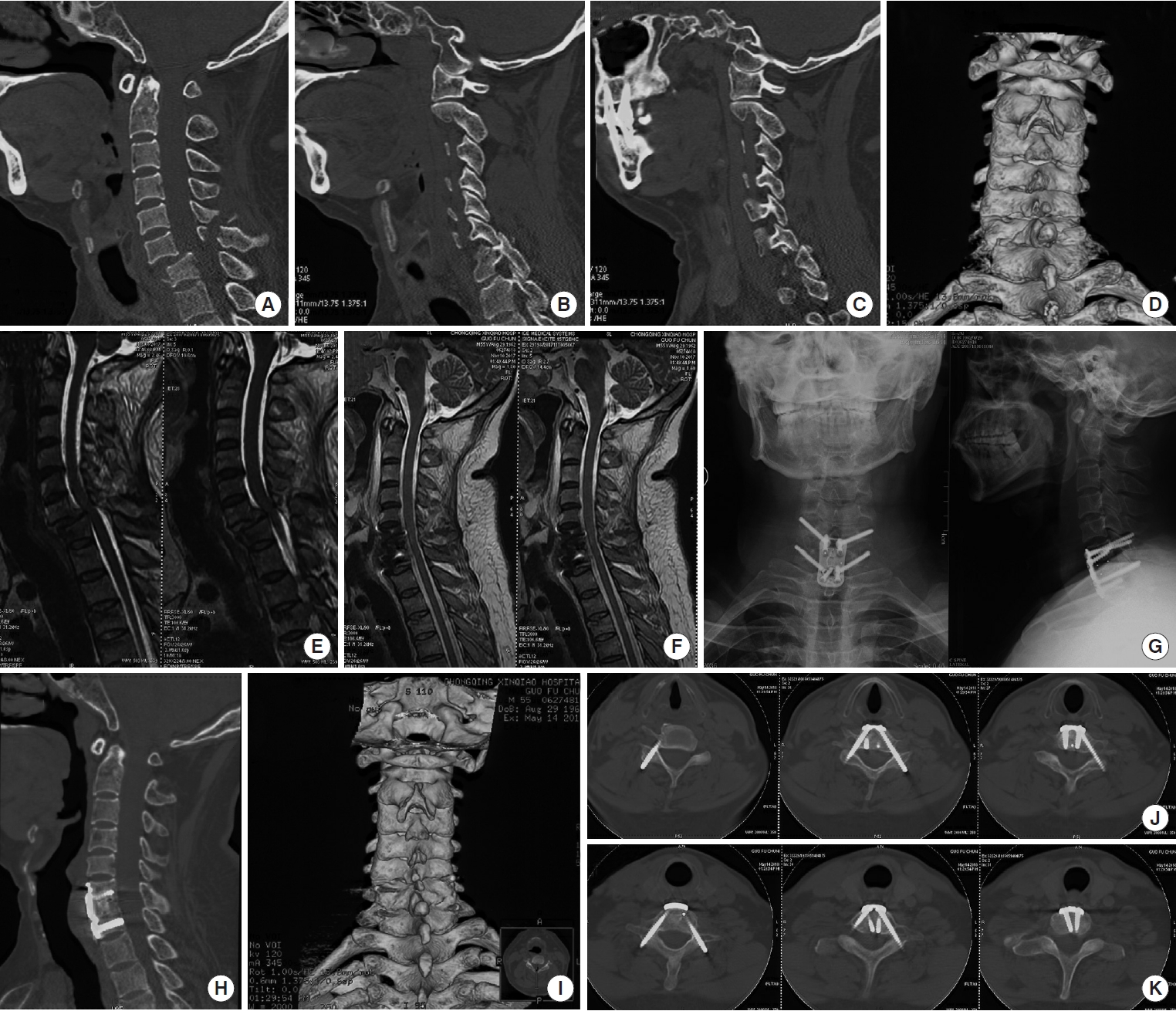
Although anterior-only approach surgery has many advantages [41] (Table 2), for some patients with delayed dislocations, it is difficult to open the facet joints directly with anterior-only approach techniques. In order to release the facet joints, the weight of traction is often given too much to them, which may cause secondary iatrogenic injury to the spinal cord. Especially, for patients with severe vertebral fractures or osteoporosis, they cannot even withstand the force of distracting provided by the spreader. Johnson et al. [61] described a 13% radiographic failure rate for anterior plate fixation in patients with flexion injuries of the subaxial cervical spine in 2004. They postulated that facet fractures might have an impact on the stability of anterior plate fixation. Amorosa and Vaccaro [62] also recommended that for patients with severe posterior column injury, the stability was not good enough after anterior surgery alone, which needed to add posterior fixation. Alternatively, the anterior pedicle screw and plate fixation reported by Zhang et al. [63] can also be used, so that the anterior-only approach can also meet the stability of the 3 columns (Fig. 11). However, this surgical technique is challenging and requires a highly experienced surgical team.
2. Posterior-Only Approach Techniques
Posterior surgery is advocated because of its ease of reduction and restoration of the cervical spine alignment. After cervical spine trauma, the biomechanical advantages of posterior fixation and the high stability of cervical pedicle screw fixation have been reported. Especially for patients with posterior column damage, posterior reduction and fixation can provide higher stability than anterior approach [64-66]. For patients with old facet dislocation, severe vertebral fractures, osteoporosis, ankylosing spondylitis, or comminuted fractures of the facet joint, it may fail to reduction using anterior-only approach techniques. Therefore, some authors recommend performing posterior surgery directly or adding posterior fixation after anterior surgery [61,67,68].
Historically, posterior open reduction was performed most frequently, and the technique consisted of instrument-assisted manipulation, a partial or complete facetectomy, reduction of deformity and dorsal fixation, and fusion. Fusion and instrumentation techniques included facet wiring, interspinous wiring, and placement of a lateral mass plate or pedicle screw rod system [6,69-78]. Especially for the reduction techniques with instrument-assisted manipulation, there were various instruments, including periosteal elevator, spinal curette, bone-holding forceps, pedicle screws and so on. In 1967, Alexander et al. [69] firstly reported the reduction technique assisted by a small sharp periosteal elevator (Adson). In the state of skeletal traction with Crutchfield tongs, a small sharp periosteal elevator was inserted between the facets, and gradually turned and twisted it until the separation between the two becomes wider and adhesions have been broken up. In some instances, if the adhesions could not be broken up, the ventral margin of the involved superior facet, or even the whole facet, might have to be removed to complete the reduction. Subsequently, using the same principle of leverage, Bunyaratavej et al. [79] in 2011 and Park et al. [80] in 2015 respectively reported a similar mean assisted by the spinal curette. A small straight spinal curette was placed between the inferior facet of the rostral vertebra and the superior facet of the caudal vertebra. With gentle pressure and a twisting maneuver, the curette tip would slide between them. The curette was then turned so that the cup side docked with the inferior edge of the rostral facet. Care must be taken not to place the tip of the curette more deeply than the inferior edge of the rostral facet to avoid injuring the exiting nerve root, which was located near the inferior edge of the rostral facet. The handle of the curette was then gently pulled caudally so that the rostral facet is levered up and over the caudal facet (Fig. 12).
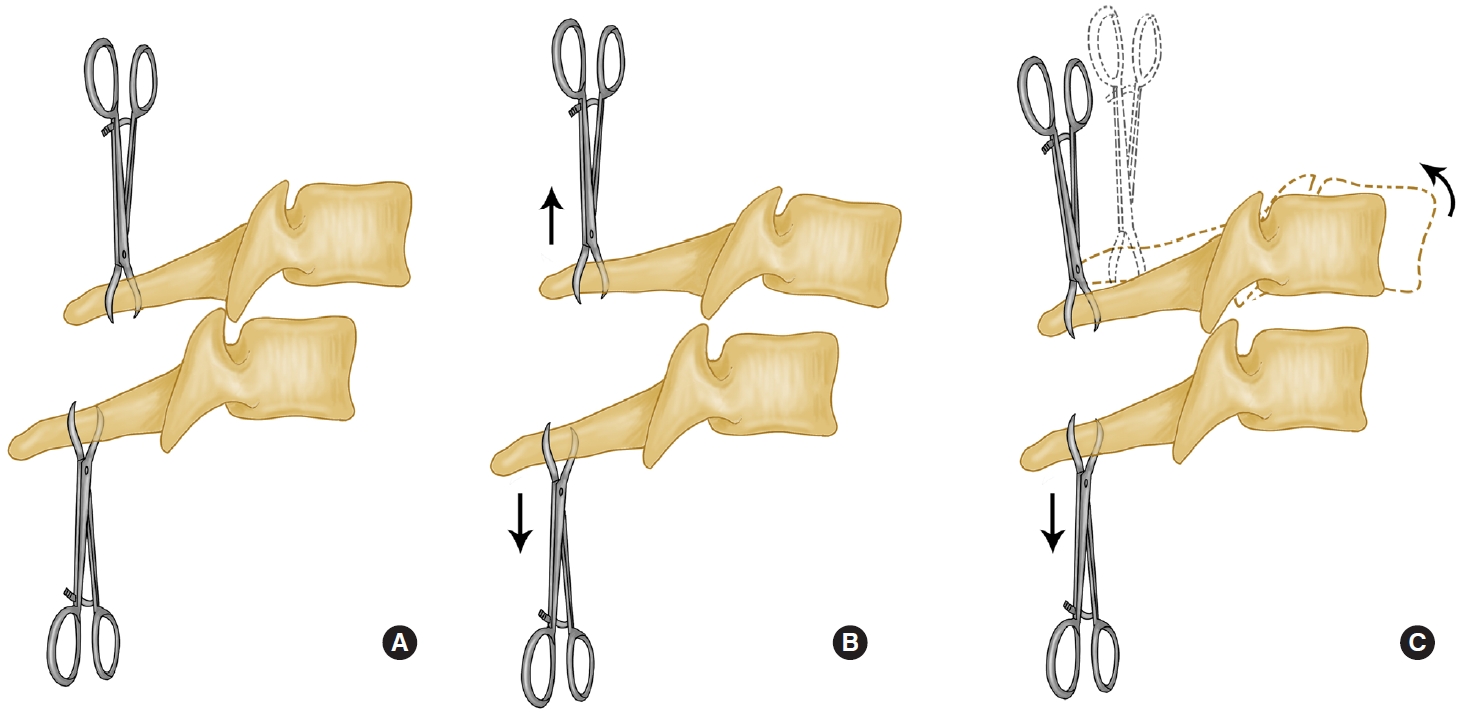
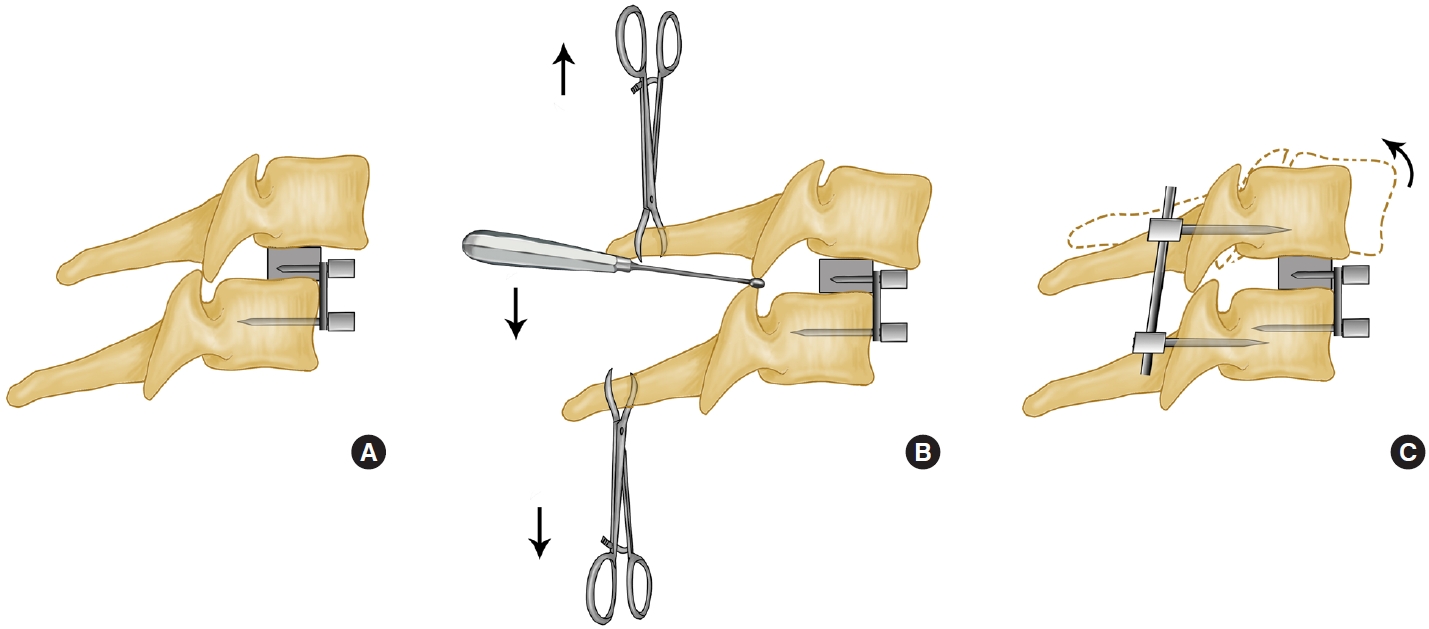
Some authors who considered that some patients of cervical facet dislocation might combine with traumatic disc herniation, proposed that neurological damage would occur if we reduced the injured spine without adequate distraction force [81]. In 2001, Fazl and Pirouzmand [82] described a new technique for dorsal reduction of facet dislocations by use of a modified interlaminar spreader. As the same principle, Nakashima et al. [81] reported the use of bone-holding forceps for posterior reduction in the treatment of 40 patients with cervical fracture-dislocations and traumatic disc herniation in 2010. Firstly, axial traction was gently applied to the injured cervical spine using the Mayfield head holder before operation. After exposure, in cases of dislocation or subluxation, a distraction force was gradually applied between the spinous processes, using bone-holding forceps, to reduce anterior translation of the proximal vertebra. When the inferior articular process of dislocated vertebrae was just right on top of the superior process of inferior vertebrae, a dorsal force was pulled to the rostral vertebra to achieve reduction (Fig. 13).
If reduction could not be achieved, especially for old cervical subluxation, a high-speed burr might be used to release the locked facets by resection of the tip of the superior articular process of the distal segment. In 2014, Barrenechea [83] reported a 1-stage posterior technique utilized in the reduction of high-grade lumbar spondylolisthesis to reduce an old cervical subluxation. Under neurophysiologic monitoring, the patient was placed in a Mayfield head holder with her neck slightly extended. After opening and exposing the posterior elements, the locked C5ŌĆō6 facets appeared ossified. they performed a wide bilateral foraminotomy using a high-speed drill to refracture the partially ossified facets. And then, they placed 6 lateral mass screws (2 on C4, 2 on C5, and 2 on C6) followed by securing a rod from C4 to C6, spanning the C5 lateral mass screw. Resembling the technique utilized in the reduction of high-grade lumbar spondylolisthesis with ŌĆ£reduction screws,ŌĆØ they used a rod reducer to bring the C5 screw head back toward the rod, thus realigning the lateral mass screw heads and reducing the subluxation (Fig. 14).
Compared with anterior techniques, posterior techniques can directly release the locked facets, which is easier to reduce, and can also remove the compression on the dorsal side of the spinal cord (Table 3). Moreover, posterior pedicle screw fixation has better biomechanical stability which can provide more favorable conditions for long-term bone graft fusion [84,85]. However, the posterior-only surgery has its serious drawbacks: (1) The herniated intervertebral disc and other soft tissues on the ventral side of the spinal cord cannot be removed before reduction; (2) During the reduction of the posterior approach, the compressive materials may enter the spinal canal and compress the spinal cord, which bring iatrogenic surgical complications; (3) Patients with intervertebral disc destruction may be at risk of poor fusion rate and internal fixation failure due to lack of support for the anterior-middle column. Thus, a further anterior procedure should be considered in cases with canal compromise with traumatic intervertebral disc herniation [86].
3. Combined Approach Techniques
Combined anterior and posterior fixation/fusion is the most definitive operation to maintain cervical stability after a fracture or dislocation, and this has been demonstrated by many authors in biomechanical experiments or clinical studies. Therefore, it has been more recommended for the treatment of a bilateral dislocation than anterior or posterior fixation/fusion alone, which are more accepted in unilateral dislocation [87-89].
Because of reduction via the posterior approach is less challenging than that via the anterior approach, almost all the reduction techniques used by the authors are from the posterior approach mentioned before, and the only difference is the sequence of the surgical approach. There are many ways of combined approach surgery, including anterior-posterior, posterior-anterior, anterior-posterior-anterior, and posterior-anterior-posterior approaches. In 2008, Liu et al. [90] reported a novel operative approach for the treatment of old distractive flexion injuries of subaxial cervical spine. They firstly performed facetectomy and released sufficient soft tissue for reduction, fixed with spinous process wire, and used morselized autogenous cancellous graft harvested from the posterior iliac process to posterior element fusion through a posterior approach. And then an anterior approach surgery was performed for decompression, fusion and internal fixation. Thereafter, there have been more authors who recommend posterior-anterior order used posterior lateral mass screws or pedicle screws for fixation [91,92]. In recent years, with the advancement of minimally invasive techniques in recent years, considering that traditional posterior surgical trauma will bring complications such as neck pain, some authors have used minimally invasive techniques to achieve posterior release and reduction. In 2019, Shimizu et al. [93] reported a fluoroscopy-assisted posterior percutaneous reduction technique for the management of unilateral cervical facet dislocations. The reduction instrument and principle were the same as those reported by Alexander et al. [69] in 1967, except that Shimizu et al. [93] inserted the elevator into the locked facet percutaneously through a small incision above the facet with fluoroscopic assistance, and reduction was achieved by lever action without complications. Subsequently, Yang et al. [94] reported 4 cases of old subaxial cervical facet dislocations unlocked by the posterior approach under endoscopy followed by anterior decompression, reduction, and fixation.
However, cases have been reported of patients who were neurologically intact before intraoperative reduction, but who experienced a deficit after the reduction [30,95]. Some authors recommend anterior discectomy first, and if the reduction can be obtained by means of the anterior incision, the anterior column can be grafted and fused using standard techniques. If required, this procedure can be followed by posterior fusion and instrumentation. There have been many studies of anterior-posterior surgery in recent decades [96-99]. Feng et al. [100] described a surgical technique of anterior decompression and nonstructural bone grafting followed by posterior reduction and fixation in 2012. The patients were firstly placed in the supine position. After discectomy through a standard Smith-RobinsonŌĆÖs anterior cervical approach, the Caspar distraction pins were placed divergently in a rostrocaudal fashion and the disc space was distracted 1 to 3 mm to restore near-normal disc height and to correct the kyphosis. A layer of absorbable gelatin sponge was gently filled into one-third of the posterior disc space to protect the exposed spinal cord and prevent dislocation of cancellous bone graft. Afterwards, a layer of morselized cancellous bone grafts from the iliac crest was placed in two-thirds of the anterior disc space, restoring proper intervertebral height and lordosis. Then a layer of gelatin sponge was placed on the surface of bone graft, and the longus colli muscle was opposed over the sponge and stitched carefully. The anterior wound was closed and turn to prone position, and then the posterior reduction and internal fixation of the lateral mass screws were performed (Fig. 15).
On the other hand, if the reduction cannot be succeeded through the anterior approach, a posterior approach must be used to obtain the reduction, which leaves a question of how to address the anterior fusion and instrumentation. Often, after posterior reduction and fusion, the anterior column is approached again to place a bone graft in the disc space and affix a plate, requiring yet a third procedure to complete the treatment. This technique was rarely used in the past because of its complicated procedures and complications. Bartels and Donk [101] reported the anterior-posterior-anterior approach and posterior-anterior-posterior approach for the treatment of delayed traumatic bilateral cervical facet dislocation in 2002.
In order to avoid the third procedure, some authors applicated some new means of anterior bone grafting. In 2001, Allred and Sledge [102] described a technique for grafting and instrumentation of the anterior cervical spine before reduction using tricortical iliac crest bone graft secured with a buttress plate. In 2013, Song et al. [103] considered that the buttress plate did not provide safety from graft motion or impingement of the spinal cord since it did not completely fix the interbody graft. Therefore, they reported a modified technique using a prefixed polyetheretherketone cage and plate system. Similarly, Wang et al. [104] reported a novel surgical approach, which was successfully applied to treat 8 cervical facet dislocation patients. After anterior discectomy, a suitable peek frame cage, containing the autologous iliac bone particles or tricalcium phosphate bone substitute, was inserted in the position to fill the interspace. And then, by using 2 screws, an appropriate anterior peek composite buttress plate was added to fix the cage to the lower vertebral body. The anterior wound was closed, and the patient was placed carefully in the prone position for the posterior manipulation. Reduction of the facet dislocations was gradually achieved by gentle distraction of the involved spinous processes with tooth forceps and prying the locked facets with a reset handle, as well as positioning the patientŌĆÖs neck progressively into extension at the same time. Finally, posterior internal fixation was performed using mass screws or pedicle screws (Fig. 16).
Combined approach surgery has the both advantages of anterior-only approach and posterior-only approach (Table 4). However, the sequence of combined approach is still controversial. The sequences and techniques of surgical decompression and fixation need to be determined according to the specific conditions of the patient. The procedure is more complicated than anterior-only or posterior-only approach, which requires a higher physical condition of patient and results in a higher risk of postoperative infection. Furthermore, multiple changes of position may even cause secondary spinal cord injury.
CONCLUSION
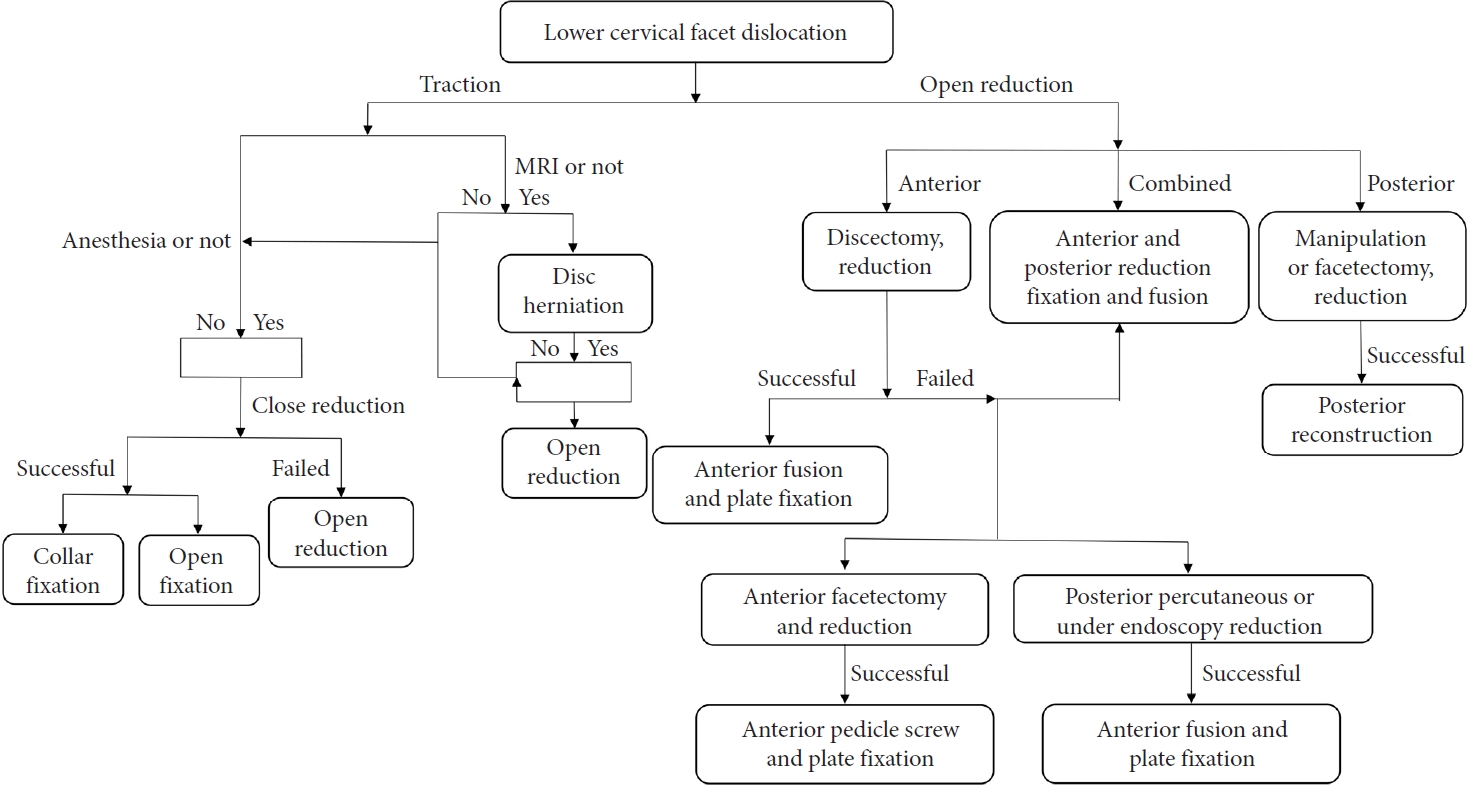
Although there were many treatment strategies and algorithms in the past [42,105,106], the optimum treatment strategy and algorithm of cervical facet dislocation is still a matter of debate (Fig. 17). Despite agreement in the literature over the role of closed reduction and surgical treatment of these injuries, there are still areas of debate including indications for MRI and MRI timing. The selection of surgical approach depends on a combination of factors, including surgeon preference, patient factors, injury morphology, and inherent advantages and disadvantages of any given approach [42,107].
















")













