







INTRODUCTION
Chiari malformation type I (CMI) is characterized by caudal tonsillar herniation and is closely associated with the development of syringomyelia [1]. Suboccipital decompression is the preferred treatment for adult patients with CMI and syringomyelia [2-4]. Decompression surgery aims to restore cerebrospinal fluid (CSF) circulation and relieve nerve tissue compression around the foramen magnum; however, the method of decompression is not standardized, and many questions remain unanswered [5]: Is bony decompression alone (BD) sufficient? When is duraplasty required? How should the resolution of syringomyelia be evaluated? Although numerous studies have investigated the considerable benefits and drawbacks of subdural procedures [6], most of the studies found that the type of decompression surgery is selected based on the surgeon’s proficiency [3,7]. Furthermore, tools for the prognostic assessment of CMI (especially syringomyelia) need to be improved and standardized, as these potentially affect the evaluation and communication of the outcomes of decompressive surgery. In the majority of studies, the three-dimensional nature of syringomyelia has been neglected as single-level parameters have been used to represent syringomyelia [8,9].
This study evaluated the intraoperative findings in CMI patients with syrinx according to individualized, tailored surgical procedures, wherein decompression was considered complete when a free CSF pulse was observed. Based on the percentage of postoperative change in cervical syrinx volume, we intended to develop a novel scale to assess syringomyelia resolution.
MATERIALS AND METHODS
1. Participant Population and Data Collection
This retrospective observational study included patients with primary CMI and syringomyelia who underwent first-time decompression surgery in the neurosurgery department from February 2014 to April 2022. This study was approved by the Institutional Review Board of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (JS-3414). The inclusion criteria enabled the selection of symptomatic adult patients (≥ 18 years) with CMI (including borderline CMI [10]) and syringomyelia with comprehensive medical and imaging records. Patients who were younger than 18 years, diagnosed with other CM types (II, III, or IV) or secondary syrinx (caused by spinal cord tumor, trauma, etc.) or secondary tonsillar hernia (caused by intracranial hypertension, etc.), accompanied by skeletal anomaly (such as basilar invagination, or scoliosis) were excluded. The control group included symptomatically and radiologically asymptomatic volunteers for Chiari and syringomyelia. Based on their clinical presentation, including symptoms related to CSF obstruction (Valsalva- or strain-induced occipital/upper cervical pain/headache), symptoms related to compression/dysfunction of brainstem, cerebellar, or cranial nerves (swallowing difficulty, downbeat nystagmus, autonomic symptoms, trigeminal/glossopharyngeal neuralgia, etc.), and symptoms related to spinal cord dysfunction (pain and temperature sensory loss, motor weakness, spasticity, etc.), participants were classified under 3 categories (Supplementary Table 1) [3].
Two neuroradiologists assessed the T2-weighted magnetic resonance imaging (MRI) sequences of all participants and the mean values of their results were calculated. Image files were downloaded in the Digital Imaging and Communication in Medicine format and converted for markup and measurements using ITK-snap v25.0 (http://www.itksnap.org/pmwiki/pmwiki.php). The midsagittal T2-weighted imaging of the cervical spine was used to measure the tonsillar herniation distance, tonsillar descent distance, cerebral aqueduct diameter, and pB–C2 line (Fig. 1). Tonsillar herniation was measured as the distance between the lowest points of the tonsillar and basion-opisthion line. Tonsillar descent was defined as the distance between the lowest points of the tonsil and the line drawn from the top of the dorsum sella to the internal occipital protuberance. The anteroposterior cerebral aqueduct diameter was measured at the level of the inferior margin of the corpora quadrigemina. The pB–C2 measurement methodology has been described previously [11]. Briefly, the pB–C2 line was drawn as the longest perpendicular distance from the B–C2 line (the line through the posteroinferior tip of the clivus and posteroinferior corner of the C2 vertebral body) to the ventral dura. The level of origin of the syrinx and the region of cord involvement (cervical, thoracic, or lumbar) were assessed and recorded. The cervical syrinx volume was obtained using the T2-weighted axial sequences of the cervical spine and measured as the volume of the syrinx above the C7 level (Fig. 2).
2. Surgical Procedure
The same 2 experienced neurosurgeons, who worked in cooperation with each other in our institution, performed all procedures to avoid any surgical biases. Patients were placed prone and the position was secured with 3-point pin fixation. A midline incision was made from the inion down to the spinous process of C2. The midline avascular plane was disconnected with monopolar electrocautery and retracted to expose the C1 posterior arch and the occipital squama. After suboccipital craniectomy (approximately 3 cm× 2 cm) and C1 laminectomy, the outer layer of the dura mater was removed, and the neurosurgeons decided whether a dural opening was necessary. If the free CSF pulse could be observed through the inner layer of the dura in the operative region, decompression was done and the incision was closed (posterior fossa BD [PFD] group). If there was no free CSF pulse observed, a Y-shaped opening was made in the dura. If the free CSF pulse of the cisterna magna and the outlet of the fourth ventricle was inspected through the dural opening, an autologous fascia (harvested from the occipital pericranium) was used to ensure a watertight sealing of the dura to facilitate adequate decompression; great care was taken to preserve the intactness of the arachnoid during duraplasty (PFD with duraplasty [PFDD] group). Alternatively, the arachnoid membrane overlying the cisterna magna and the outlet of the fourth ventricle was opened. To gain access to Magendie’s foramen and enter the fourth ventricle, the tips of the cerebellar tonsils may be retracted laterally. Next, the adhesive arachnoid veil or scarring blocking the obex was removed until pulsatile CSF circulation was visible from the central canal (PFDD with additional obex exploration [PFDDO] group). The neck muscles are gently approximated for closure and the fascia was closed to ensure complete closure. The patient was monitored postoperatively in the intensive care unit for a day or 2 and then transferred to the ward. The postoperative complications that were reported din this study cohort included meningitis, CSF leakage, and poor wound healing.
3. Outcome Assessments
The postoperative outcomes of decompressive surgery were evaluated using the Chicago Chiari Outcome Scale (CCOS) system [12]. The percentage change of the cervical syrinx volume on MRI was measured using the following formula: [(preoperative cervical syrinx volume – postoperative cervical syrinx volume) × 100%]/preoperative cervical syrinx volume. The scale used to ascertain the change in the percentage of cervical syrinx volume was based on the volume determined at the last radiological follow-up. Patients with grades I, II, and III had less than 30%, 30% to 70%, and more than 70% improvement in volume, respectively. The prognosis was considered an ordinal variable, wherein higher grades indicate better odds of syringomyelia resolution. The CCOS score was calculated from the records of the patient’s last follow-up.
4. Statistical Analysis
All analyses were done using IBM SPSS Statistics ver. 25.0 (IBM Co., Armonk, NY, USA). The categorical variables were described using the frequency count. The mean± standard deviation and median (interquartile range) were used to define normal and abnormal distribution continuous variables, respectively. The intraclass correlation coefficient (ICC) was used to determine the agreement between 2 independent raters. A multivariate linear regression model was developed to investigate variables that independently affect the CCOS. Moreover, a multivariable ordinal regression model was established to investigate these variables, with syrinx prognosis as the outcome of interest. The p-values were obtained from the models. Statistical significance was defined by a 2-tailed p < 0.05.
RESULTS
1. Sample Characteristics
A total of 78 individuals who were diagnosed with CMI and syringomyelia underwent decompression surgery (Table 1) were included in our cohort; 76.9% of participants were female, and the median age in the cohort was 43.50 years. The most common presenting symptoms were related to spinal cord dysfunctions (82.1%), and 50% of patients had the classic symptom of head and neck pain. Moreover, in 68 patients (87.2%), the syrinx originated above C3, and in 54 patients (69.2%) the syrinx extended to thoracic or lower levels. There was no significant difference in the overall preoperative characteristics of the 3 decompression groups (Table 1). The ICCs of all measurements indicated minimal interobserver variability (all ICCs >0.75) (Supplementary Table 2).
2. Tonsillar Descent and Tonsillar Herniation
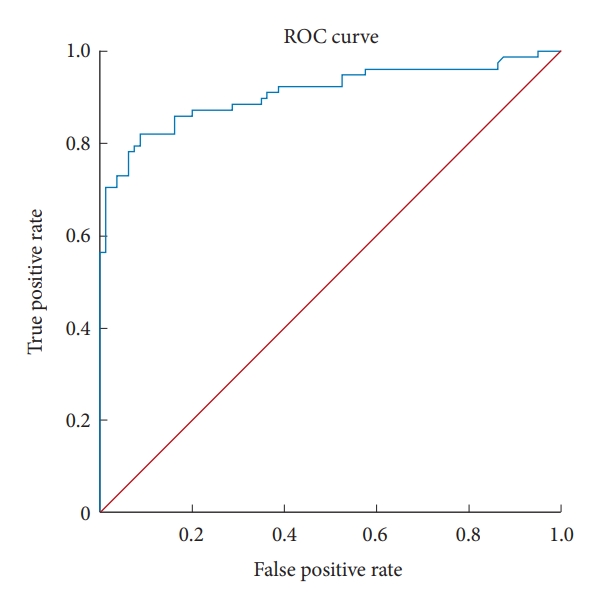
Correlation analyses showed a strong positive correlation of tonsillar herniation with tonsillar descent (p < 0.001 for both) (Supplementary Table 3). Eighty healthy volunteers (53 female; median age, 41.50 years) were recruited as the control group (Table 2). After coordinating the most acceptable sensitivities and specificities, a cutoff at 36.93 mm was determined and the efficacy of the tonsillar descent to diagnose CMI achieved an area under the ROC of 0.909 (78 CMI patients and 80 controls; 95% confidence interval, 0.860–0.958; p < 0.001) (Fig. 3). Thus, considering that the McRae line no longer existed due to the removal of occipital squama, it was acceptable to assess the tonsillar resolution using the tonsillar descent value. Preoperative tonsillar descent and pB–C2 values were significantly higher in CMI patients than in healthy controls (p < 0.001 for both) (Table 2), which indicated a lower tonsil position and more severe vetral brainstem compression in CMI patients.
3. Surgical Outcomes of the Entire Cohort
After decompression, the tonsillar shrunk and the cerebral aqueduct diameter decreased significantly (Tables 2, 3); 29.5% of patients exhibited a reduction of cervical syrinx volume of more than 70%, whereas 57.7% had a more than 2-mm resolution in tonsillar descent (Table 3). At the last follow-up, the median CCOS score of the total patients was 15 points, and 88.5% of patients achieved an improved CCOS score (13–16 points). In 1 patient (1.3%), pain and nonpain symptoms worsened and necessitated a revision surgery at another hospital. Specifically, the median score for pain relief, nonpain symptom relief, functionality, and complications were 4, 3, 4, and 4 points, respectively. The median follow-up period was 73 months, and the median period for radiological follow-up was 5 months.
We found no significant intergroup difference in tonsillar descent resolution (both value and scale), cervical syrinx volume resolution (both value and scale), and CCOS (both value and scale; p > 0.05 for all). The PFDDO group demonstrated a trend of achieving more favorable CCOS and pain scores.
4. Determination of Radiological Measurements Grading
The distribution in our adult group was 4 (5.13%), 38 (48.72%), and 36 (41.15%). Based on the Grabb classification, the pB–C2 readings of young CM patients were classified into low (6 mm), medium (6–9 mm), and high (> 9 mm) readings [13]. The preoperative average pB–C2 measurement of our cohort was 8.73 mm. Grabb et al. [13] found that CMI patients with pB–C2 less than 9 mm had better outcomes following posterior decompression. Thus, we divided the patients into 2 groups as follows: pB–C2 line < 9 mm (distribution, 42/78) and ≥ 9 mm (distribution, 36/78) (Table 1).
The average aqueduct diameter has previously been reported to be less than 2 mm [14]. In our cohort, the median aqueduct diameter was 1.75 mm for CMI patients and 1.70 mm for healthy controls. Therefore, we divided the patients into 2 groups as follows: aqueduct diameter < 1.8 mm (distribution, 45/78) and aqueduct diameter ≥ 1.8 mm (distribution, 33/78) (Table 1).
Furthermore, we classified the cervical syrinx volume resolution into three comparably sized groups based on appropriate measures of central tendency as follows: volume resolution ≥70% (distribution, 23/78), volume resolution=30%–70% (distribution, 28/78), and volume resolution < 30% (distribution, 27/78) (Table 3).
5. Multivariate Analysis on CCOS Score
Multivariate analysis using clinically relevant variables demonstrated that patients with younger age at surgery (Beta=0.034, p = 0.018), without symptoms of CSF obstruction (Beta=-1.150, p = 0.001), syrinx originating from lower cervical levels (Beta=1.182, p = 0.037), narrower preop aqueduct (Beta=1.117, p = 0.005), and better syrinx volume resolution scale (Beta=0.701, p = 0.004) showed an independent association with a higher CCOS score (Table 4). Although not statistically significant, a more invasive surgical procedure may provide patients with better CCOS (Beta=0.241, p = 0.230) (Table 4).
6. Multivariate Analysis on the Syrinx Resolution
Multivariate analysis using clinically relevant variables demonstrated that patients with higher CCOS scores (odds ratio [OR], 1.555; p = 0.017), narrower preoperative aqueduct (OR, 3.341; p = 0.035), and better tonsillar descent resolution (OR, 4.052; p = 0.007) showed an independent association with a better cervical syrinx volume resolution scale (Table 5). The follow-up period seemed to affect both the CCOS score and the syrinx resolution scale (Tables 4, 5). The CCOS score may worsen during the follow-up period (Beta=-0.004), whereas syrinx resolution may improve over time (OR, 1.060); however, the results were not statistically significant (p = 0.471 and p = 0.073, respectively). Moreover, different surgical procedures did not significantly affect the cervical syrinx resolution when decompression options were individualized for each patient; however, intradural operations tended to be more effective for improving cervical syrinx as compared to PFD.
DISCUSSION
1. Pathophysiological Changes in CMI
Understanding the pathophysiology of Chiari malformation (CM) and syringomyelia is essential for identifying potential factors that are associated with the surgical outcome. However, the extent to which the low position of the tonsil is physiological, the factors that fundamentally cause tonsillar herniation, and the strategy for defining the neuroradiologic criteria of CMI remain unelucidated [10]. As asymptomatic patients remain asymptomatic during follow-up, most neurosurgeons only consider symptomatic patients for surgery. Thus, the diagnosis of CMI is based more on a functional definition than on an anatomical diagnosis of tonsillar herniation ≥ 3–5 mm [15]. Although a small posterior fossa in comparison to the volume of the cerebellum is widely considered as underlying the cerebellar tonsils extending through the foramen magnum, this feature may not be present in all patients [16].
This study compared the preoperative tonsillar herniation length, cerebral aqueduct diameter, and pB–C2 between CMI patients and control cohorts to identify CM-specific features morphologically and physiologically. The size of the tonsillar herniation, by definition, represents the extent of herniation. Measurements of the pB–C2 line on midsagittal images have been used to reflect ventral cervicomedullary compression objectively [11,13]. Morphological measurements of the cerebral aqueduct did not change with age and sex [14]. We used the aqueduct diameter to describe the conditions of CSF flow and neurodegeneration above the fourth ventricle. Measurements of the posterior cranial fossa vary, and none of them reflect the 3-dimensional morphology of occipital squama. In our clinical experience, we have encountered an occipital bone that inclined straight as though the tonsillar would slope inferiorly through it as well as a more horizontally or even tipped-up occipital bone that uplifts the tonsillar structure [17]. Although patients with associated bony anomalies were excluded from our cohort, the pB–C2 in patients with CMI was more significant than in healthy controls; this suggests that the pB–C2 may be a potential pathogenic factor in CM. Furthermore, the preoperative aqueduct diameter of the CMI patients did not differ significantly from that of controls. This may be due to the exclusion of concomitant hydrocephalus in our cohort, which indicated that CSF disturbances above the fourth ventricle occur as a secondary effect of CMI.
2. Effect of Surgery on Morphologic Structures
The treatment strategy for CMI should focus on normalizing the pathophysiological changes. The current study found that different decompressions decreased the tonsillar size but not the pB–C2 distance. Although the predictive value of preoperative pB–C2 has not been fully established, it is widely accepted that CSF flow and tissue compression alterations contribute to CMI symptoms [3,11,18]. Grabb et al. [13] suggested that a longer pB–C2 may necessitate ventral decompression in the pediatric cohort. Consistently, Goel et al. [19] suggested that atlantoaxial instability contributes to the pathogenesis of CMI, even without apparent bone anomalies in the craniocervical junction, and recommended atlantoaxial fixation in all CMI patients. However, the effect of fixation on surgical outcomes remains controversial [20]. Diffusion tensor imaging demonstrated significant microstructural alterations in the lower brainstem and cerebellum of CMI patients compared to healthy controls, symptomatic CMI patients compared to asymptomatic CMI patients, and CMI patients with syrinx compared to those without syrinx [21,22]. However, these studies did not identify any predictive value of TBI.
3. Decompressive Options
Suboccipital decompression is generally accepted as the preferred treatment for CMI, with or without syrinx. Nonetheless, there are various surgical techniques to achieve this, and there is no consensus on the standard operative procedure. In the last century, invasive procedures such as fourth ventricle opening or obex manipulation have been associated with high mortality rates, with neurosurgeons subsequently eschewing these procedures [23,24]. Indeed, surgeons should maximize the benefits for patients while minimizing surgical complications. However, the last 2 decades have seen advances in surgical techniques and instruments, and subdural and even intra-fourth ventricle procedures are performed by experienced surgeons and are considered safe and sometimes necessary [8,24].
Debate regarding the appropriate timing and necessity of dural opening and arachnoid dissection persists. Some researchers believe that decompression should be thorough, dura should be opened in every case, and any arachnoid scar tissue encountered during the decompression should be removed. Therefore, these decompression surgeries were performed in accordance with the anatomical subtypes [24-26]. However, the surgical outcomes for CMI (and syrinx) differ with the pathological subtypes [24]. Additionally, excessive arachnoid manipulation may increase the risks of postoperative scar and hygroma formation, which can affect long-term CSF flow and may cause hydrocephalus in some cases [27].
Other researchers including the present authors, propose individualized surgical approaches based on intraoperative observation. As CMI is a functional condition and decompression aims to provide sufficient CSF flow, we support functional surgery to achieve adequate decompression according to intraoperative findings. Notably, different pathological subtypes of CMI induced similar outcomes in terms of symptoms and syrinx. “The threshold is the place to pause”: it would be even better if objective signs to indicate complete decompression were elucidated. McGirt et al. [28] suggested adequate decompression of the subarachnoid spaces assessed using intraoperative ultrasonography and showed comparable surgical outcomes between BD alone and BD with duraplasty (without opening the arachnoid), where the overall revision rate was 7% and the risk of symptom recurrence was significantly higher in the ultrasonography-guided BD-alone group. Although the revision in our cohort was 1.3% and there were no significant differences in the surgical outcomes (tonsillar descent resolution, cervical syrinx volume resolution, and CCOS) between the three surgical groups. Then, Milhorat and Bolognese [29] noted that color doppler ultrasonography was invaluable for surgical decision-making when the dura was intact; they confined their patient-specific decompression and indicated optimal CSF flow parameters for subdural operations; however, the surgical outcomes were not mentioned. Phase-contrast MRI revealed significantly different intraoperative CSF and tonsil dynamics [30]. However, the dynamic parameter still needs to be standardized.
Lower age was a protective factor for prognosis in our adult cohort. As adult CMI patients age, their surgical outcome scores consistently decline [31], and this decline may be attributed to decreased anterior CSF space with aging and makes decompression more challenging [32]. Thus, early decompression is recommended for symptomatic adult CMI patients [33]. According to the definition of CCOS, patients without pain symptoms definitely had more favorable improvement on the pain symptoms [12]. Moreover, syrinx originated from the lower cervical level and significantly achieved higher CCOS scores in our cohort. Postoperatively, the upper syrinx position was considerably lower than its preoperative level, and this indicated a less severe condition for syrinx from the lower cervical level [4]. The current results showed that a narrower aqueduct of sylvius was associated with higher CCOS scores. The aqueduct area was larger, and the aqueduct stroke volume was higher in CMI patients with syrinx than in those without syrinx [34]. A wider aqueduct may indicate greater disturbances of CSF flow above the fourth ventricle. Interestingly, tonsillar herniation secondary to hydrocephalus is always associated with aqueduct stenosis, which results from the external compression of the mesencephalon [35]. However, the pB–C2 line had no significant effect on the CCOS score. This may be attributable to the fact that Grabb et al. [13] divided participants into three roughly equal subgroups, whereas we divided our cohort into two roughly equal subgroups.
On the other hand, our findings align with those of proponents of “anatomical decompression,” although the trends of CCOS deterioration over time and CCOS improvement with the more invasive surgical procedure were not significant [24]. It is reasonable to assume that with a more extended follow-up period, the effect of our “functional decompression” may demonstrate a significantly better prognosis with more invasive procedures. Furthermore, as we had excluded bony anomalies from our CMI cohort, additional considerations may be necessary for cases with CMI and associated deformities.
4. Association Between Clinical Parameters and Syringomyelia
The correlation between syrinx resolution and postoperative symptom relief of CMI remains inconclusive [2,8,24]. Moreover, especially with the “advantage” of publication bias, more invasive surgeries seem to have trends to resolve the syrinx better. However, there is no standardized measurement method for syringomyelia resolution, and most previous studies have focused on describing the syrinx resolution at a single level [24,36]. Thus, we used the three-dimensional volume changes of cervical syringomyelia to indicate the syringomyelia resolution.
Our findings suggested that cerebellar tonsillar shrinkage was positively correlated with the prognosis of the volume of cervical syringomyelia. CMI patients with syrinx had a more inferior tonsillar herniation in terms of length than those without syrinx [37]. Our findings are consistent with the widely accepted theory of syringomyelia pathogenesis presented by Oldfield et al. [38] and Greitz [39], which identifies an exaggerated downward pulsation of the cerebellar tonsil as one of the principal contributing factors. Then, the current results showed that a cerebral aqueduct with an anteroposterior diameter of less than 1.8 mm served as a protective factor for syringomyelia resolution. A narrower aqueduct diameter may indicate a less severe CSF disturbance transmitted through the foramen magnum [35,40]. Nonetheless, this poses another question: besides the decompression procedure, what may promote the shrinking of the cerebral tonsil? Although previous studies have shown equal effectiveness on syringomyelia improvement between tonsillectomy and decompression alone [41,42], recent multicenter research has indicated that syringomyelia relief in width was more significant in patients who underwent tonsillectomy compared to those who underwent BD plus duraplasty [7]. These results highlight the need for a standard multidimensional prognosis assessment scale for syringomyelia.
5. Limitations
The study has several limitations, including its single-center design, nonrandomized-controlled retrospective design, and relatively short radiological follow-up period. Thus, the rationality and practicability of the current syrinx volume resolution classification warrants further investigation. Additionally, the study did not consider quantitative neurophysiological data corresponding with intraoperative findings and the measuring of the cervical spine. These are essential parameters that require further investigation.
CONCLUSION
Our study revealed that an individualized decompression strategy ensured comparable treatment outcomes for different CMI patients with syringomyelia. Furthermore, our novel syringomyelia resolution scale was positively correlated with Chiari outcomes, suggesting its potential use in predicting outcomes of decompression. This study guides intraoperative decision-making between PFD, PFDD, and PFDDO for CMI patients undergoing their first-time decompression surgery. Early functional decompression is recommended for symptomatic adult CMI patients, and tailored practical decompression methods provide similar surgical effects for different CMI patients. The novel cervical syringomyelia resolution scale strongly correlates with the CCOS score. Further studies are necessary to evaluate the regional anatomical and neurophysiological parameters of different subtypes of CMI patients.












")













