INTRODUCTION
Cervical disc herniation can be treated by anterior or posterior decompression. Sequestrated cervical disc can migrate to the anterior, posterior, and lateral aspect of the spinal canal. The migrated disc into the epidural space is associated with myelopathy and cervical radiculoplathy5). Anterior cervical discectomy and fusion (ACDF) is the gold standard for the management of cervical disc herniation. However, cervical corpectomy is sometimes required to remove the sequestrated disc at posterior part of vertebral body8). To avoid corpectomy, several authors have described the "transvertebral" or "transcorporeal" approached, which enable treatment without bone fusion1,6,7). We reported the treatment of such a case with a combined anterior approach without corpectomy.
CASE REPORT
A 50-year-old male presented with pain of his posterior neck, as well as his left shoulder, arm, and leg. His symptoms had developed 1 month previously. Recently, a subjective weakness in the right lower extremity had developed. Physical examination revealed increased deep tendon reflexes, and both Hoffmann's sign and ankle clonus were positive. He had taken medications of non-steroidal anti-inflammatory drugs and undergone physical therapy and acupuncture. Magnetic resonance (MR) images demonstrated a huge herniated disc compressing the left paramedian area of the spinal cord from C6-7. The ruptured disc had originated from the C6-7 disc and upwardly migrated to the C5-6 disc space (Fig. 1). Although the standard surgical management of this would have required the corpectomy of C6, we attempted to avoid cervical corpectomy. However, transcorporeal herniotomy requires a wide bone removal and it is difficult to remove the disc from the C6-7 disc space. We therefore decided to combine an ACDF with a transcorporeal herniotomy.
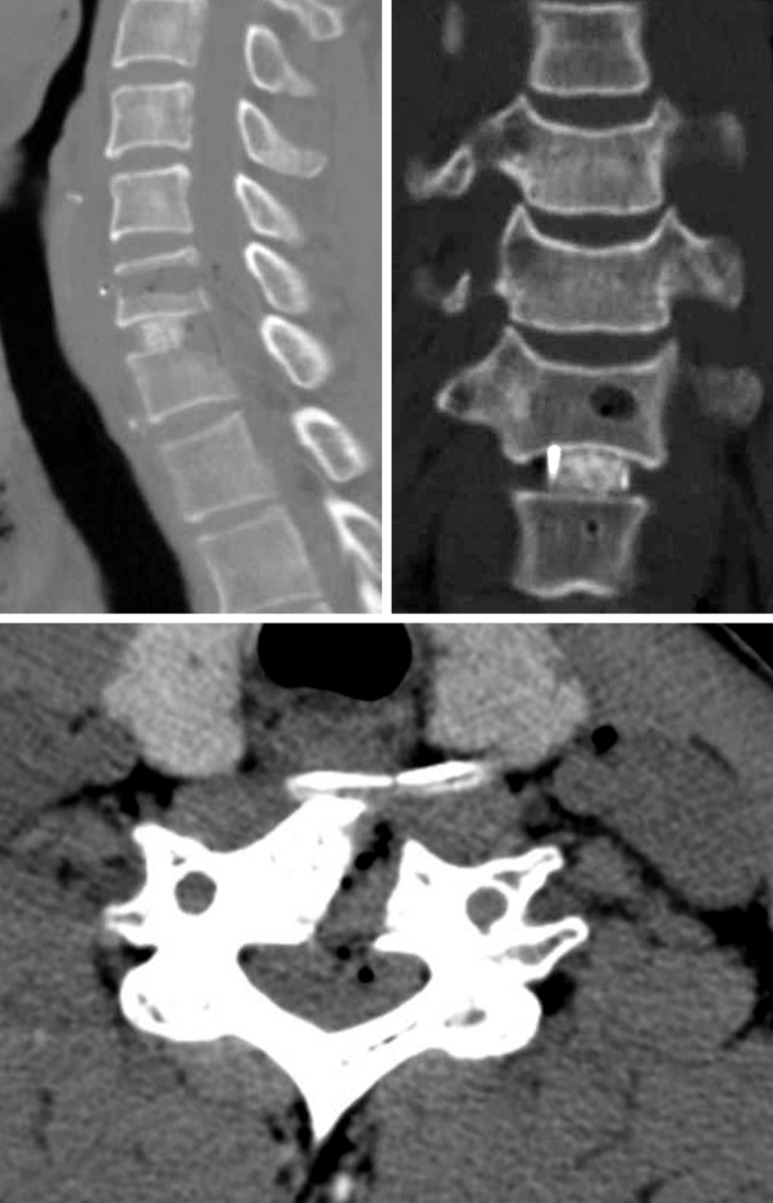
Through the Smith-Robinson approach, the disc spaces of C5-6 and C6-7 were exposed. Firstly, a cranial Caspar pin (Aesculap, Tuttlingen, Germany) was inserted into the superior left paramedian C6 vertebral body (VB), which was used as a trancorporeal approach hole. Another caudal pin was inserted into the C7 VB. The C6-7 disc and subligamentous herniated disc were removed. We tried to extract the upwardly migrated disc with a right-angled probe. However, the narrow operative field that included the C6 and C7 VBs were obstacles to its removal. Then, the cranial pin hole was widened in the perpendicular lateral direction. The posterior longitudinal ligament (PLL) was removed, after which the herniated disc fragment could be visualized clearly and removed. No fragments remained, and adequate decompression was verified with the use of a right-angled probe. After the decompression, the interbody cage was inserted into the C6-7 disc space (Fig. 2). Postoperatively, the pain and weakness experienced by the patient preoperatively was resolved. Postoperative MR and CT images revealed the total removal of the herniated disc and a well decompressed spinal cord (Fig. 3, 4).
DISCUSSION
Sequestrated cervical disc migrates not only superiorly or inferiorly in front of the cord but also compresses the cord and nerve root medially or laterally. It is important to differentiate only sequestrated disc compressing the cord from extraligamentous herniation in connection with PLL. The free sequestrated fragment is frequently found to be two or three pieces5). So, partial or complete corpectomy is required for a migrated cervical disc herniation posterior to the adjacent vertebra. The corpectomy can not miss the fragment behind the vertebral body and maintain good alignment. However, corpectomy results in an increase of the mechanical stress on the adjacent segments, which requires the sacrifice of two disc spaces including adjacent healthy disc and gives an increased complication rate, including the possibility of pseudarthrosis and subsidence2,3,4). Nakai et al. introduced the transvertebral herniotomy for the management of herniated cervical discs6). The herniated disc was removed through drilling the adjacent vertebral body. The optimal indication for this technique is a large localized herniation without spinal stenosis. Shim et al. also achieved a successful result with a transcorporeal approach for an upper cervical disc herniation7). However, in this case we concerned about removing the anterior column. This was highly likely to cause hemorrhage that would be difficult to control due to the narrow operative field after the disc fragment was removed. In particular, a huge migrated disc herniation from the index disc space to an adjacent disc space, as observed in the present case, would require wide bone resection and the index disc could not be preserved if the removal of the herniated disc was complete.
CONCLUSION
The combined anterior approach of ACDF and transcorporeal herniotomy could not only remove the disc completely with minimal bone resection and preserve the adjacent disc, but also facilitate the control of any epidural bleeding. A huge migrated cervical disc that has herniated can be removed completely with this combined approach, avoiding corpectomy.