




INTRODUCTION
Minimally invasive spine surgery may allow for surgery of the lumbar spine with considerably less blood loss and soft tissue damage. Recently, to reduce the adverse effect of the open technique of pedicle screw, the percutaneous pedicle screw fixation (PPF) is becoming more widespread in spinal surgery. Many studies about PPF have been reported, but still, there are rare reports about the result of multilevel (Ōēź3 levels) PPF4,10,12,18). This study analyzed the clinical, radiological, and surgical results of the multilevel PPF in various lumbar spinal diseases.
MATERIALS AND METHODS
1. Patient population
From March 2008 to April 2011, a total of 17 patients of lumbar spinal disease underwent neural decompression, interbody fusion and multilevel PPF by one neurosurgeon. There were 8 men and 9 women with a mean age of 61.4 years (range, 25-84) and a mean follow-up period of 23.2 months (range, 18-43).
Below is a group list of our indications for the procedure.
1) Multilevel degenerative diseases such as spinal stenosis, spondylolisthesis (Grade I), or instability with symptoms refractory to conservative treatment.
2) Severe bone destruction with a spinal cord compression or a nerve root compression due to infectious diseases such as tuberculous spondylitis or pyogenic spondylitis.
3) Spinal instability with a spinal cord compression or a nerve root compression due to trauma.
Out of 17 patients, 7 patients were degenerative diseases (5 spinal stenosis with instability, 2 spondylolisthesis), 6 patients were infectious diseases (4 pyogenic spondylitis, 2 tuberculous spondylitis) and 4 patients were burst fractures with thecal sac compression and instability (Table 1). The patients, with excessive spondylolisthesis or severe spinal deformity such as scoliosis, kyphosis, and rotational deformity, were excluded from PPF procedure.
2. Procedures and instruments
We performed neural decompression and interbody fusion first. The posterior lumbar terbody fusion (PLIF) with facectectomy via midline incision was performed in 9 patients, the posterior lumbar currettage and interbody fusion in 5 patients, and the anterior lumbar corpectomy and interbody fusion in 3 patients. Allograft iliac bone, mesh cage containing allograft bone chips, or polyetheretherketone (PEEK) cage containing allograft bone chips were used in interbody fusion.
And then, multilevel PPF was performed in prone position using CD Horizon® Longitude® (Medtronic Sofamor Danek, Memphis, TN,USA), CD Horizon® Sextant® II (Medtronic Sofamor Danek, Memphis, TN, USA), Viper® II (DePuy Spine, Raynham, MA, USA), or AnyPlus® (GS Spine, Santa Cruz, CA, USA). The screws were placed percutaneously using fluoroscopic guidance. The cannulated screws, which were inserted over a guide wire, had extenders attached to them, which had a slot to receive the rod. Since the entry point of screw insertion in the middle pedicle is most important for alignment of spine, the insertion of screw in the middle pedicle was carried out lastly.
The slot was large enough in the unreduced position to accept a rod that was passed again percutaneously. The rod is contoured according to the sagittal contour desired and then passed free hand through the slots under direct fluoroscopic control. Once the rod is appropriately positioned through all the screw extender slots, the extender is reduced to seat the rod into the tulip of the screw head. Once reduced, the top locking nut is inserted to fix the rod to the screw starting from the caudal screw and working proximally in sequential fashion. Once all the nuts are in place, the extender is unseated and detached from the screw. Compression or distraction can be applied to the extenders as desired, to gain further correction.
The average PPF level was 3.7 (range, 3-6).
3. Outcome parameters
A retrospective review of clinical, radiological, and surgical data was conducted.
Of the back pain or leg pain, the severity of main symptom was recorded using visual analog scale (VAS). Functional outcomes were measured using the Oswestry Disability Index (ODI) scores, and patient's satisfactions were recorded using Odom's criteria during follow-up period.
For radiological evaluation, we examined the dynamic X-rays, magnetic resonance imaging (MRI), and computed tomography (CT) prior to surgery, and also, the dynamic X-rays and CT consecutively during follow-up period.
The accuracy of screw position was analyzed by immediate postoperative CT. In CT scan, screw perforation of any aspects of cortex was checked, and when all parts that constitute the screw were located in pedicle and vertebral cortex, it was considered as screw accurately inserted.
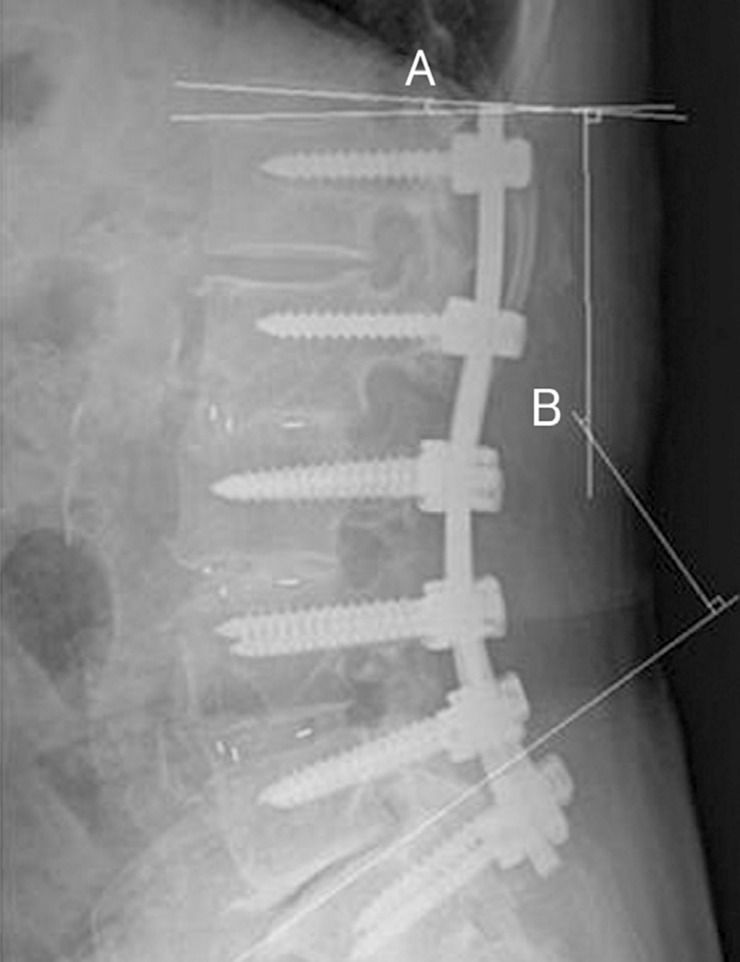
To evaluate sagittal alignment, total lumbar lordotic angle (TLA) was measured on lateral radiograph in neutral position, and adjacent segmental angle (ASA) was measured on flexion-extension view(Fig. 1). We defined definite change of ASA on the standing lateral film as sagittal translation of the adjacent vertebral body above fused level greater than 3mm and/or ASA greater than 10 degrees19). TLA and ASA were checked at the preoperative period, 1 month after the operation, 6 months after the operation, and the last follow-up.
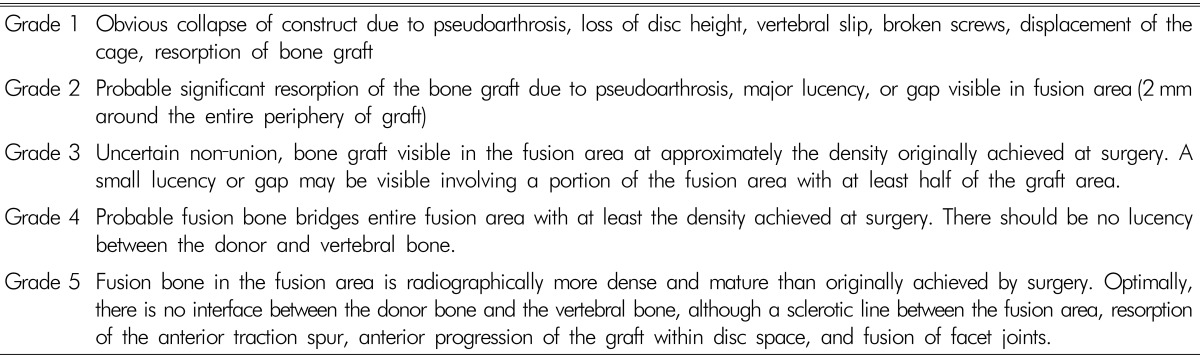
The bony fusion rate of interbody fusion and screw failure such as fracture or loosening were evaluated by dynamic X-rays and CT during follow-up period. The degree of bone fusion was based on the classification of Brantigan and Steffee2) (Table 2), and we regarded Grade 4 or 5 as a state of bone fusion. The screw loosening was confirmed when we observed more than 1mm thick radiolucent zone (halo sign) around screw on plain radiographs. Also, we have identified the development of the late postoperative complications such as instability and instrument failure.
Surgical outcomes were evaluated by checking the operation time, estimated blood loss (EBL), duration of postoperative bed rest and length of hospital stay. The occurrence of perioperative morbidities such as neurologic deterioration, cerebrospinal fluid (CSF) leakage, wound infection, pneumonia, heart problem, urinary difficulty, epidural hematoma, and deep vein thrombosis were checked. Also, we tracked the frequency of reoperation.
RESULTS
1. Clinical outcomes
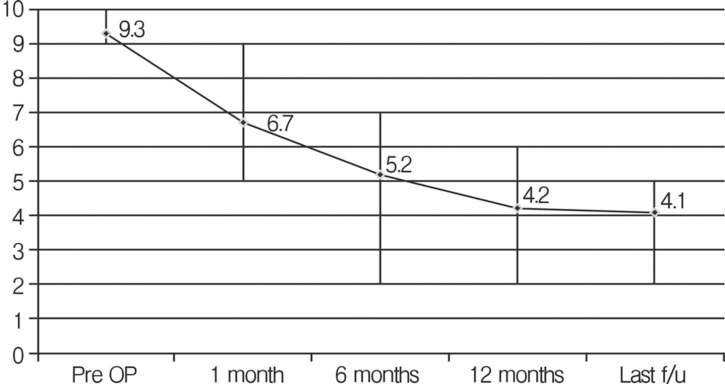
The mean VAS score at the 1 month after the surgery 6.7 (range, 5-9) was significantly lower than the preoperative score, 9.3 (range, 9-10). The mean VAS score decreased at each follow-up evaluation and was significantly lower at the last follow-up 4.1 (range, 2-5) compared with the preoperative score (Fig. 2).
The mean ODI score also improved from 71.2 (range, 67-81) preoperatively to 38.0 (range, 29-61) at the last follow-up (Fig. 3). Both VAS and ODI score improved after the surgery and the improvement maintained during the follow-up period with statistical significance (p<0.05).
According to the Odom's criteria, the results were excellent in 6 patients (35.3%), good in 7 patients (41.2%), and fair in 4 patients (23.5%) at the 6-month follow-up, and excellent in 7 patients (41.2%), good in 8 patients (47.0%), and fair in 2 patients (11.8%) at the last follow-up. Therefore, the clinical success rate according to the Odom's criteria was 88.2%(Fig. 4).
2. Radiological outcomes
In all the patients, by CT scan immediately after the surgery, the cases of screw malposition were 6 (4.1%) out of 146 screws. However, there was no occurrence of neurological deficit or vascular complications, and also no need of screw correction.
The mean TLA increased from 34.7┬░ before the surgery to 38.0┬░ at the 1 month after the surgery, however, decreased to 35.9┬░ at the last follow-up. The mean ASA was 5.7┬░ at preoperation and 7.0┬░ at the last follow-up. The mean ASA of the caudal adjacent segment was 5.6┬░ at pre-operation and 5.3┬░ at the last follow-up. There was no statistical significance in the changes of the TLA and ASA. Only 2 patients (11.8%) showed definite change of ASA of cranial adjacent segment, and all of them were asymptomatic.
During follow-up period, there were bony fusions in 15 patients out of 17 patients who underwent interbody fusion, and thus fusion rate was 88.2%. On the other hand, there were screw loosening in 2 patients, but there was no pull-out or fracture of screw. Among 2 patients of screw loosening, 1 patient showed progressive lumbar kyphotic change without aggravation of symptom, and 1 patient showed instrument related infection and underwent removal of screw at 1 year after the surgery.
3. Surgical outcomes
The mean operation time was 5.9 hours (range, 5.0-9.5), EBL was 550ml (range, 300-1,500) with need of average 1.2 packs (range, 0-4) of transfusion, and duration of bed rest was 2.0 days (range, 1-4). The mean length of hospital stay was 26.4 days (range, 8-59), which was longer period than expected, maybe due to long-term antibiotic therapy for infectious patients. Except for 6 infectious patients, mean length of hospital stay was 13.6 days (range, 8-22).
Fortunately, there was no major perioperative morbidity except for a single case of reoperation for resolving hemoperitoneum in patient who underwent anterior corpectomy and fusion.
DISCUSSION
The pedicle screw fixation has been used as a universal spinal fusion surgery method for many spinal disorders. Standard open technique for pedicle screw fixation, however, has been associated with several disadvantages. During the open technique, extensive tissue dissection and longtime retraction are inevitable to expose entry points of screw and to provide orientation of lateral to medial for optimal screw trajectory. The excessive retraction of muscle can cause ischemic damage and permanent pathological changes of the muscle7,8,20,21). Already, some authors reported that the degree of damage of muscles and back pain after surgery were proportionate to the size and time of retraction during surgery5,17). In addition, extensive dissection of paraspinal muscle can cause excessive blood loss and necrosis of tissue, which can be said to increase the need for transfusion and the chance of postoperative infection20). Such problems cause longer bed rest duration, lengthy hospital stay, and significant cost22). Moreover, some authors have suggested that the open technique can cause adjacent segment degeneration due to extensive dissection of paraspinal muscle or iatrogenic injury of facet joint14,19).
As these problems become important matter, recently, minimally invasive PPF was introduced and developed. PPF uses small muscle splitting approach to allow placement of hardware under fluoroscopic guidance. This technique permits accurate hardware placement while avoiding adverse effects of open technique. Based on this concept, many authors have reported about advantages of single- or two-level PPF such as shorter operative time, less paraspinal muscle damage, less need for postoperative oral analgesics, and lower blood loss than open technique9,13). For multilevel (more than 3 levels) PPF, the longer the length of rod is more difficult to insert, and adjusting alignment of pedicle is difficult. However, recently, with introduction of new instruments, multilevel PPF method that can do a wide range of spinal fusion was developed. Multilevel PPF has usually been carried out for degenerative scoliosis patients1, but it is still not widely carried out yet, and so the clinical result of the operation method are not known well.
The results of the author's present study demonstrated favorable clinical and radiological outcomes. In the current study, with regard to patient's symptom and satisfaction, improvement of clinical outcomes such as VAS and ODI were significant. Also, radiological outcomes including rate of screw malposition (4.1%), fusion rate (88.2%), occurrence of definite change of ASA(11.8%), and occurrence of screw looseing (11.8 %) were satisfactory. Although it is difficult to compare our results with the other studies because there are many factors affecting outcomes, such as the patient's medical condition, surgeon's experience, surgical indication, surgical method, and outcome assessment criteria, the outcomes in the present study are comparable to other reports11,23).
Multilevel lumbar fusion surgery is needed for multilevel decompression and spinal stability. However, in some special cases, the choice of multilevel fusion is cautious. For example, elderly patients may be at increased risk of surgical morbidities such as pneumonia, cardiovascular event, or wound infection. Also, the patients with medical comorbidities such as cardiovascular disease, renal disease, and diabetes may represent a significant challenge for surgery. The open technique for multilevel fusion, which has the disadvantage of increased operative time and blood loss, may not be tolerated in these elderly patients with poor preoperative general conditions. However, multilevel PPF can be tolerable in even these patients. Compared to the literature6,16), based on surgical outcomes of current study, we can demonstrate multilevel PPF to be technically feasible, to be accomplished within tolerable operative times, to be associated with less blood loss than the open technique, and to be associated with short hospital stays. Moreover, there was no surgical complication except for a single case of reoperation due to hemoperitoneum.
Despite all the above, limitations of multilevel PPF have been described, including steep learning curves and theoretically increased radiation exposure3). Also, in rare cases, the inserted instrument comes to be positioned close to skin, which can cause serious skin stimulating symptom, and so instrument removal is needed15).
With development of various instruments of multilevel PPF, it is possible to insert contoured long rod as required for the spinal curvature, and to correct malalignment by compression or distraction. However, the indication is more limited than open technique. In cases of the significant malalignment of pedicle before the surgery due to severe spondylolisthesis (Grade II or more), severe scoliosis, or rotational deformity, it is difficult to carry out reduction of spinal curvature with percutaneous method. Also, since this surgery is carried out under C-arm fluoroscope, the pedicle should be within the range of anatomical structure that can be predicted under fluoroscope by the performing physician. For example, in cases of excessive degeneration and formation of osteophyte, it is hard to find pedicle under fluoroscope, and so accurate test is necessary and attention should be paid before the surgery. Moreover, as the shape of rod which is inserted percutaneously is limited in lordotic or mild kyphotic curved form, it is difficult to apply for severe kyphotic deformity. So, as mentioned above, patients with excessive spondylolisthesis or severe spinal deformity were excluded from this multilevel PPF.
There are some limitations to the present study that should be dealt with. This study was retrospective and had a small patient group with too short follow-up period. Furthermore, the study population is heterogeneous with varying indications for spinal fixation, and there is no comparison with open techniques. Additional study is required to compare the multilevel PPF to the open technique in cases of identical operative indications.
CONCLUSION
Using newer posterior percutaneous instruments, it is possible to achieve multilevel PPF for various lumbar spinal diseases, with favorable clinical, radiological, and surgical outcomes. It remains to be seen whether long-term outcomes are also favorable. Also, the preoperative pedicle alignment is an important factor in multilevel PPF.













")













