




INTRODUCTION
Infectious spondylodiscitis (SD) is an infection of intervertebral discs and adjacent vertebral bodies7,10). Various organisms including bacteria, tuberculosis, fungi, and parasites can cause SD7). In the past, tuberculosis infection was the major cause of spinal infections5,7,10,15). However, nowadays, the majority of spinal infections are bacterial monomicrobial5,7,9,15). Staphylococcus aureus, Escherichia coli, Proteus, Klebsiella, Pseudomonas aeruginosa, Coagulase negative Staphylococcus, streptococci, enterococci, and Mycobacterium tuberculosis were discussed as common pathogens in majority of literatures3,5,6,9,11,13,14,15,18,20). Empirical antibiotics have been used to focus on these common pathogens. Unfortunately, uncommon pathogens could be unresponsive to these empirical antibiotics resulting in treatment failure.
There are case reports on spinal infections cause by individual uncommon pathogens, but large studies encompass uncommon pathogens are rare. The goal of this study is to evaluate the prevalence of SD by uncommon pathogens and the efficacy of treatment strategy including empirical broad-spectrum antibiotics therapy in comparison with common SD.
MATERIALS AND METHODS
Ninety-nine consecutive patients treated for infectious SD in a single tertiary hospital from January 2007 to May 2015 were reviewed retrospectively. The diagnosis of infectious spondylitis was based on presentation of clinical symptoms, laboratory abnormalities (white blood cell counts, C-reactive protein, erythrocyte sedimentation rate), radiographic abnormalities, microbiological results and pathologic findings.
S. aureus, E. coli, Proteus, Klebsiella, P. aeruginosa, Coagulase negative Staphylococcus, streptococci, enterococci, and M. tuberculosis were discussed as common pathogens in majority of literatures3,5,6,9,11,13,14,15,18,20). We defined uncommon pathogens as every pathogen except the common pathogens mentioned above, that includes rare bacterial, fungal, and parasitic organisms.
Patient demographics, predisposing factors such as systemic illness and previous history of spinal procedure or surgery, etiological organisms and its sensitivity to empirical antibiotics, and clinical outcome including mortality, hospitalization day, cure rate, recurrence, and need for reconstructive surgery were analyzed to compare uncommon SD group with common SD group. Statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). The p-values were generated using Mann-Whitney test and p-values less than 0.05 were considered significant.
Each patient was treated with various antibiotics, but we assumed that they were treated with vancomycin and 3rd or 4th generation cephalosporin for the empirical antibiotics before identification of organism, which are one of the most broad spectrum antibiotics, in the analysis of the empirical antibiotics treatment efficacy. Patients with tuberculosis spondylitis (with either microbiological or radiological confirmation) were excluded from antibiotics efficacy analysis, because they tend to have unique clinical, radiological features to differentiate them from pyogenic infections, relatively sensitive diagnostic tools including acid fast stains and reverse transcription-polymerase chain reaction, and require entirely different medications7,9,15,17,20). Patients were treated for various periods of time, however, clinical improvements, normalization of inflammatory marker, improvement on imaging follow-up were required for cessation of treatment.
RESULTS
1. Patient Demographics and Risk Factors
Of 99 patients who fulfilled inclusion criteria, 55 (55.6%) were male and 44 (44.4%) were female with a mean age of 60.8 years. There were 68 cases with positive culture results, 54 of them(79.4%) were common pathogen and 14 (20.6%) were uncommon pathogen. Thirty (55.6%) were male and the mean age was 61.3 years in the common pathogen group. Ten (71.4%) were male and the mean age was 60.1 years in the uncommon pathogen group.
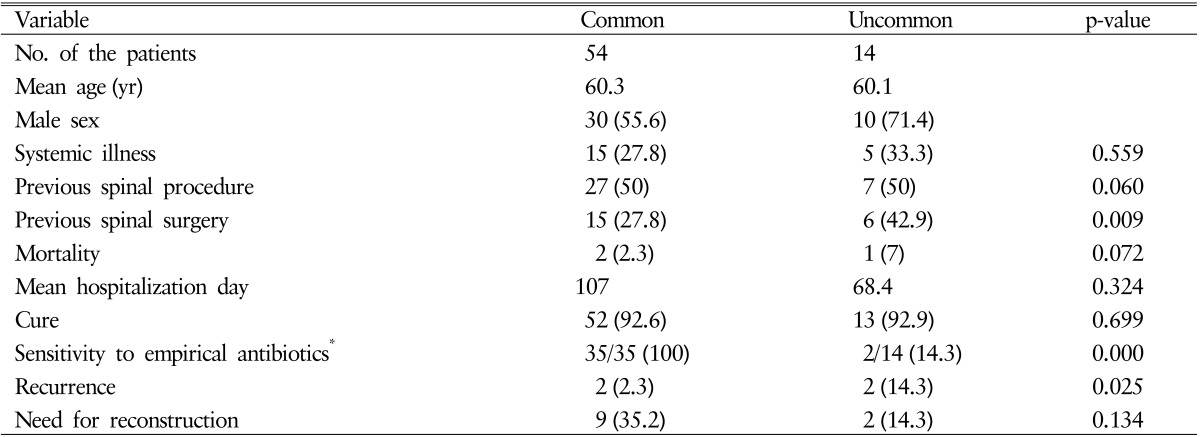
Systemic illness including diabetes, hepatic failure, Cushing syndrome, renal failure, heart failure in common pathogen group, and uncommon pathogen group were noted in 15 (55.6 %) and 5 cases (33.3%), respectively. There was no statistically significant difference (p=0.559). Twenty-seven (50%) of common pathogen group and 7 (50%) of uncommon pathogen group had history of previous spinal invasive procedures adjacent to the lesion such as acupuncture, epidural blocks, spinal anesthesia, skin grafts, catheter insertions. History of previous spinal surgery was much higher in uncommon SD group (42.9 %) than in common SD group (27.8%), and it was statistically significant (p=0.009) (Table 1).
2. Etiologic Organism
Among 99 patients, 64 had open and 35 had percutaneous (fluoroscopic or ultrasound guided) biopsies. The causative organism was confirmed by in 68 cases (68.6%). Culture positive rates for open and percutaneous procedures were 78.1%(50 of 64) and 51.4%(18 of 35), respectively.
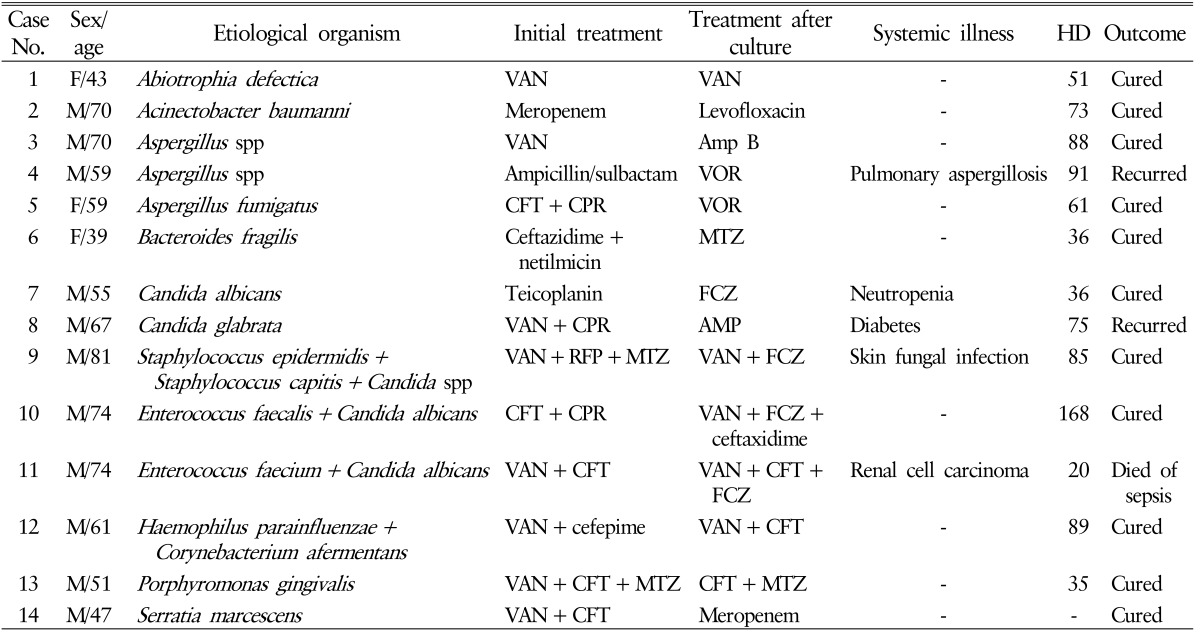
There were 14 cases (20.5% of culture positive SD and 14.1% of total cases) of SD caused by uncommon pathogens. Microorganisms were: Abiotrophia defectica, Acinectobacter baumanni, Bacteroides fragilis, Haemophilus parainfluenza with Corynebacterium afermentans, Porphyromonas gingivalis, Serratia marcescens, 3 cases of Candida with coinfected bacterial infection, 2 Candida species, 3 Aspergillus infections (Table 2).
Of 54 cases with common SD(79.4% of culture positive SD and 54.5% of total cases), 33 were bacterial monomicrobial, 2 were bacterial polymicrobial, 19 were tuberculous.
3. Treatment and Outcome
The cure rate of common and uncommon SD group was 96.3 % and 92.9%, respectively. Two patients in common SD group died of aggravated pneumonia and hepatic failure, and one patient in uncommon SD group died of sepsis. The mean duration of hospitalization was 107 days and 68.4 days for common and uncommon pathogen group. Statistical analysis showed no significant difference in mortality, cure rate and duration of hospitalization between the 2 groups (p>0.05) (Table 1).
Only 2 cases (14.3%) in uncommon SD group were covered by empirical antibiotics whereas every 35 cases (100%) of nontuberculous cases of common SD group were covered by vancomycin and 3rd or 4th generation cephalosporin (Tables 1, 2). Patients with negative culture results were treated with broad spectrum antibiotics except for 2 patients who showed typical magnetic resonance finding of tuberculosis spondylitis and treated with antituberculosis medication. All of 31 patients with negative microbiological results showed clinical improvement with the use of antibiotics.
Recurrence rate was higher in uncommon pathogen SD(14.3 %) than common SD group (2.3%), and it showed statistically significant difference (p=0.025). Reconstructive fusion operations were performed because of progressive deformity or intractable pain despite treatment for 19 (35.2%) in common SD group and 2 (14.3%) in uncommon SD group (Table 1).
4. Case Rresentation
A 59-year-old female (case number 5) with a history of discectomy 2 months before the symptom onset was transferred from local clinic with high fever and severe back pain. She was diagnosed with SD(Fig. 1A) and treated with empirical antibiotics treatment of ceftriaxone and ciprofloxacin for 3 weeks in local clinic without biopsy. Follow-up image shows aggrava- tion of the disease (Fig. 1B). Open biopsy was performed and Aspergillus fumigatus was identified. Intravenous voriconazole for 2 weeks and oral voriconazole for 9 months was administered. Reconstructive fusion operation was performed later. Eighteen-month follow-up image shows total control of the SD (Fig. 1C).
DISCUSSION
Infectious spondylitis is not a common disease, consisting 2%-7% of cases of osteomyelitis2,3,5,7). However, several studies have reported increased incidence possibly due to increasing average age, immunodeficiency, diabetes, drug abuse, various invasive procedure, spinal surgeries, and better diagnostic tools2,3,5,7,10,12).
Tuberculous SD was believed to be the leading cause of spinal infection in developing countries including Korea5,7,15). In our study, M. tuberculosis was the single most common causative organism(27.9%). Then again, bacterial pyogenic infection all together (60.3%) showed almost 2 folds higher incidence and uncommon SD (20.6%) had at least a half incidence. With the greater use of immunosuppressants, prolonged use of broad-spectrum antibiotics, indwelling catheters, and the higher prevalence of chronic debilitating diseases, the epidemiology and etiology appear to be changing8,9,19). It is also important that these once-rare pathogens can be resistant to antibiotics that are currently used1,8).
Many reports and guidelines strongly recommend identification of the pathogen before the start of antibiotics treatment, except when the patient is in a septic condition1,4,7,19). Various procedures from simple blood culture, percutaneous biopsy, and excisional biopsy to even reconstructive instrumentation can be performed. However, in our study, only 54.9% of the patients who were transferred from other hospitals were treated with various IV antibiotics without an attempt to acquire microbiological identification of the causative organism. This seems inappropriate since a considerably high portion of SD is resistant to even the most broad-spectrum antibiotics we use. In addition, such treatment can decrease the sensitivity of culture1,9).
In our study, uncommon SD was not-so-uncommon (20.5% of culture positive SD and 14.1% of total cases) within modern population, and only 14.3% of them were proved to be sensitive to vancomycin and 3rd or 4th generation cephalosporin. In addition, the ratio of presence of previous spinal surgery in uncommon SD is significantly higher than that of common SD (p=0.009), which is contrary to popular belief that etiology of postoperative infections is most likely one of skin microbiota. Positive ratio of recurrence was the only parameter with statistically significant difference between two groups in clinical outcome. Two cases (case numbers 4 and 8) recurred after cessation of parenteral antibiotics were both fungal infection (Aspergillus and Candida), which require much longer periods of treatment and recur more often. Sufficient duration of treatment and careful observation in follow-up periods are required for uncommon SD.
Physicians Should Always Consider Uncommon Pathogens With Multiple Drug Resistance, Fungal Organisms, And Polymicrobial Infections Especially When Treating Patients With Known Risk Factors Or Experiencing Treatment Failure Or Recurrence1,6,16,19). In Addition, The Importance Of Identification Of The Pathogen Before The Start Of Antibiotics Treatment Must Be Emphasized.
CONCLUSION
In our study, the prevalence of uncommon SD was relatively high uncommon (20.5% of culture positive SD and 14.1% of total cases) and the coverage rate of empirical antibiotics for them were only 14.3%. In particular, the possibility of uncommon pathogen with fungal, polymicrobial, or multiple drug resistant organism should be considered in especially when treating patients with known risk factors or experiencing treatment failure or recurrence.











")













