







INTRODUCTION
Spinal cord injury (SCI) is a destructive neurological state with complex pathophysiologic consequences. SCI often occurs secondary to trauma that leads to loss of sensory, motor, and/or autonomic functions [1,2]. The initial mechanical injury to the spinal cord causes damage to neural parenchyma, disruption of axonal networks, and glial membrane disruption, collectively known as primary injury [1]. Following this initial insult, secondary damage to the injured spinal cord may occur via apoptotic signaling, ischemia, excitotoxicity, inflammation, and axonal demyelination. Glial scar formation often develops as a result of these local events, which can impair axonal regeneration and synaptic neuroplasticity across the injury site [3]. Although there have been several improvements in the understanding of SCI pathophysiology and clinical care, there is no cure for SCI, and the current standard of treatment focuses on teaching compensation strategies to mitigate losses of function.
Recent research has demonstrated novel methods to improve post-SCI recovery and reverse the deleterious outcomes of SCI. Most cases of SCI have an intervening gap of intact tissue at the site of injury; while this tissue is anatomically intact, it is functionally silent due to disruptions to the flow of information within the spinal cord [4]. Upper motor neurons lose the feedback of afferent signals and the descending efferent signals terminate at the level of the SCI lesion, though in some cases, propriospinal connections can still provide indirect access to afferent signals [5,6]. Recent research has indicated that functional recovery can be achieved by taking advantage of the remaining neural connections to re-enable sensorimotor function [7]. In mouse models, Courtine et al. [5] show functional recovery of propriospinal relay connections can only occur when spatially separated lateral hemisections are also separated temporally (i.e., when spinal hemisections were delivered 10 weeks apart), indicating the ŌĆ£rewiringŌĆØ of connections following SCI via neural plasticity. Circuit reconstruction involves not just the growth of new nerves, but also synaptic regeneration and axonal regrowth to strengthen pre-existing sensorimotor networks [8,9]. The spontaneous formation of new synapses from local surviving terminals or distant axons occurs in neural tissue that has been spared but is responding to injury. Appropriate axonal growth can be stimulated by growth factors or genetic activation; in rats, growth cone formation and axon regeneration may improve with changes to the axonal cytoskeleton [10,11]. By modulating the microenvironment of an injury to increase synaptic regeneration or axonal regrowth, damaged neural circuits can potentially be reconstructed with variable functionality.
One technique that has recently grown in prominence for functional recovery in chronic SCI patients is the use of chronic electrical stimulation of the spinal cord. Use of spinal cord stimulation (SCS) on the lumbosacral spinal cord of individuals clinically diagnosed with chronic, motor complete SCI has demonstrated restoration of a wide range of functions. The impact of long-term implantation remains unknown and requires further study along with factors such as injury level and grade, stimulation parameters, and associated pharmacology and physical therapy, which may lead to greater efficacy. The restorative power of adjunctive SCS is likely enabled by the remaining propriospinal fibers that support plasticity by enabling communication across the spinal cord lesion. Animal and computational models have suggested that SCS may recruit nearby Group I and II afferent fibers which excite myelinated motor neurons through monosynaptic and/or polysynaptic pathways [12-15]. In rodent models, transformation from dormant to active tissue at the injury site occurs through increasing the general level of excitability, allowing sensory information to become a source of control for voluntary movement; using sensory information as a source of control requires an extensive amount of physical training to allow for appropriate remodeling of supraspinal and intraspinal pathways [16]. Further study of electrical stimulation for functional recovery in human patients with chronic SCI is necessary to determine the efficacy of such treatments and to translate electrical stimulation from basic research to effective clinical use.
The aim of this review is to discuss the efficacy and safety of SCS as a neuromodulatory strategy for restoration of neurologic function in patients with chronic SCI. Previous work has been performed to survey the scientific literature regarding the effects of SCS in SCI, however these reviews have focused on either eSCS or tSCS and their effects on a limited number of physiological systems [17]. Here, we discuss the reported effects of SCS, both epidural spinal cord stimulation (eSCS) and transcutaneous spinal cord stimulation (tSCS), on sensory, motor, autonomic, cardiovascular, and pulmonary systems. Finally, we review the limitations of the current literature, and future directions for research in this promising area. This review indicates that eSCS and tSCS are efficacious and safe treatments for chronic SCI, with the potential to improve motor and autonomic function following SCI, but further work needs to be performed to define what patients will respond most efficaciously to either eSCS or tSCS therapy.
METHODS
1. Search Strategy
To undertake this review, we followed a protocol in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [18]. A search was made of the following electronic databases: PubMed, Cochrane Registry, Embase, and OVID. For the search, we used keywords spinal cord injury, spinal cord stimulation, epidural stimulation, transcutaneous magnetic stimulation, motor control, movement, and rehabilitation, combined in the databases as follows: (ŌĆ£spinal cord injuryŌĆØ) AND (ŌĆ£spinal cord stimulationŌĆØ OR ŌĆ£epidural stimulationŌĆØ OR ŌĆ£spinal cord stimulatorŌĆØ OR ŌĆ£epidural stimulatorŌĆØ OR ŌĆ£Electrodes, ImplantedŌĆØ OR ŌĆ£paddle spinal cord stimulatorŌĆØ OR ŌĆ£implantable electrodesŌĆØ OR ŌĆ£transcutaneous magnetic stimulationŌĆØ OR ŌĆ£Spinal Cord Injuries/therapy*ŌĆØ OR ŌĆ£Spinal Cord Stimulation/methods*ŌĆØ) AND (ŌĆ£motor controlŌĆØ OR ŌĆ£movementŌĆØ OR ŌĆ£rehabilitationŌĆØ). The search was conducted from the start dates of each respective database until January 1st, 2022. Additionally, we carried out an inverse search of the references cited by any relevant articles.
2. Selection Criteria
Using the PICOS structure (Patients, Intervention, Comparison, Outcome, and Study design), we established the following inclusion criteria, requiring (1) human patients to have SCI, (2) electrical spinal stimulation to be applied, and (3) outcomes to include assessment of response. We excluded articles that (1) used spinal stimulation for chronic pain treatment and (2) present secondary data, such as literature reviews. Studies performing retrospective analysis on data collected while routinely conducting clinical protocols for evaluation of SCS for spasticity or chronic pain treatment were included. The selection of articles was decided by 2 independent researchers (AL and ES) working in parallel with no points of disagreement.
3. Study Selection
The process for selecting articles was as follows: (1) any duplicates of studies found in the various databases were eliminated; (2) after an initial screening of titles, the abstracts were read to identify articles that fulfilled the pre-established inclusion criteria; and (3) the full text of the remaining studies was read, with any studies meeting the exclusion criteria being ruled out. Researchers worked in parallel to extract data, including subject demographics and injury information as well as SCS stimulation parameters and post-SCS outcomes. Given the possibility of enrollment in multiple studies, for the sake of our review, we treated each patient enrolled in a study to be independent of other patients and other studies. For clinical trials including control groups, we excluded patients in the control groups from our analyses.
4. Bias Assessment
The risk of bias was assessed by 2 independent researchers (AL and ES) using the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) tool by the Cochrane Scientific Committee for nonrandomized studies of effects of interventions. A detailed description of the process can be found in the Supplementary Table 1.
RESULTS
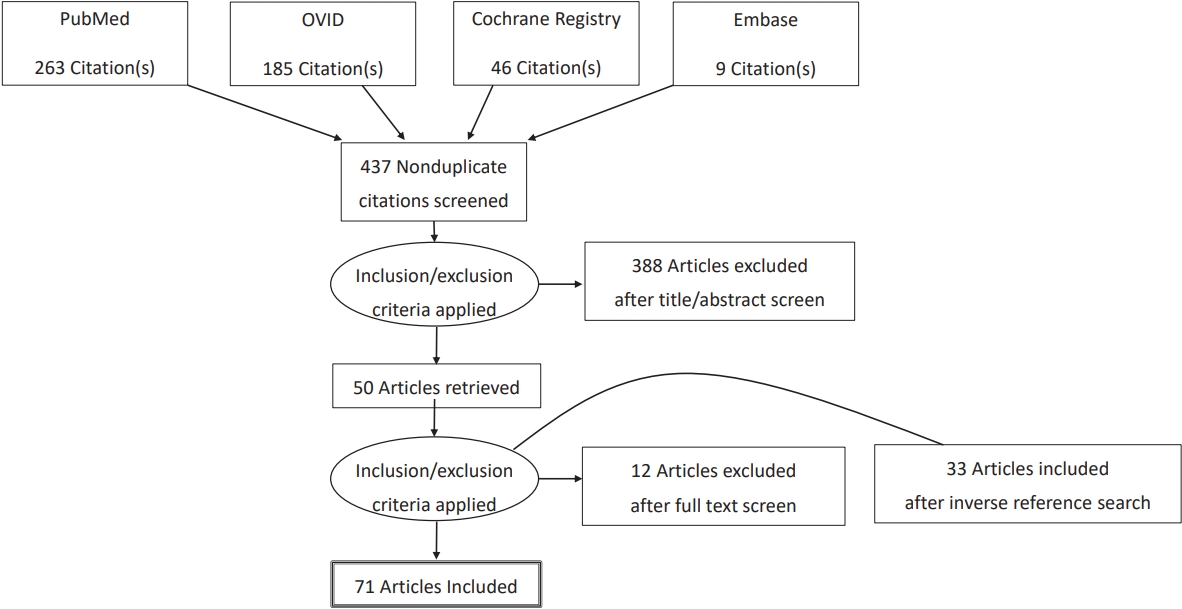
A total of 503 research reports were located in the above databases. After eliminating duplicates and screening of titles and abstracts, 50 reports were selected for a full reading of the text. After full reading, 12 articles were excluded, and 33 additional studies were identified through the review of bibliographic references. Finally, 71 studies were included in the review. The study selection process can be seen in Fig. 1.
The study design and characteristics of participants are shown in Table 1. Of the reports included in the review, 50 were case or case-series studies [2,7,19-66] and 21 were clinical trials [67-88]. The total study sample comprised of 327 patients with SCI, 257 males, 54 females, and 16 participants where sex was not specified. Patient age ranged from 18 to 66 years old. The time since injury ranged from 0.1 to 41.1 years. The majority of patients had injury levels in the cervical (n= 174 patients) and thoracic (n= 106 patients) regions. The highest reported level of injury was at C1 in a study by Estes et al. [84]. The most studied American Spinal Cord Injury Association (ASIA) scores were ASIA A (n=132), followed by ASIA B (n= 67), ASIA C (n= 40), and ASIA D (n= 29).
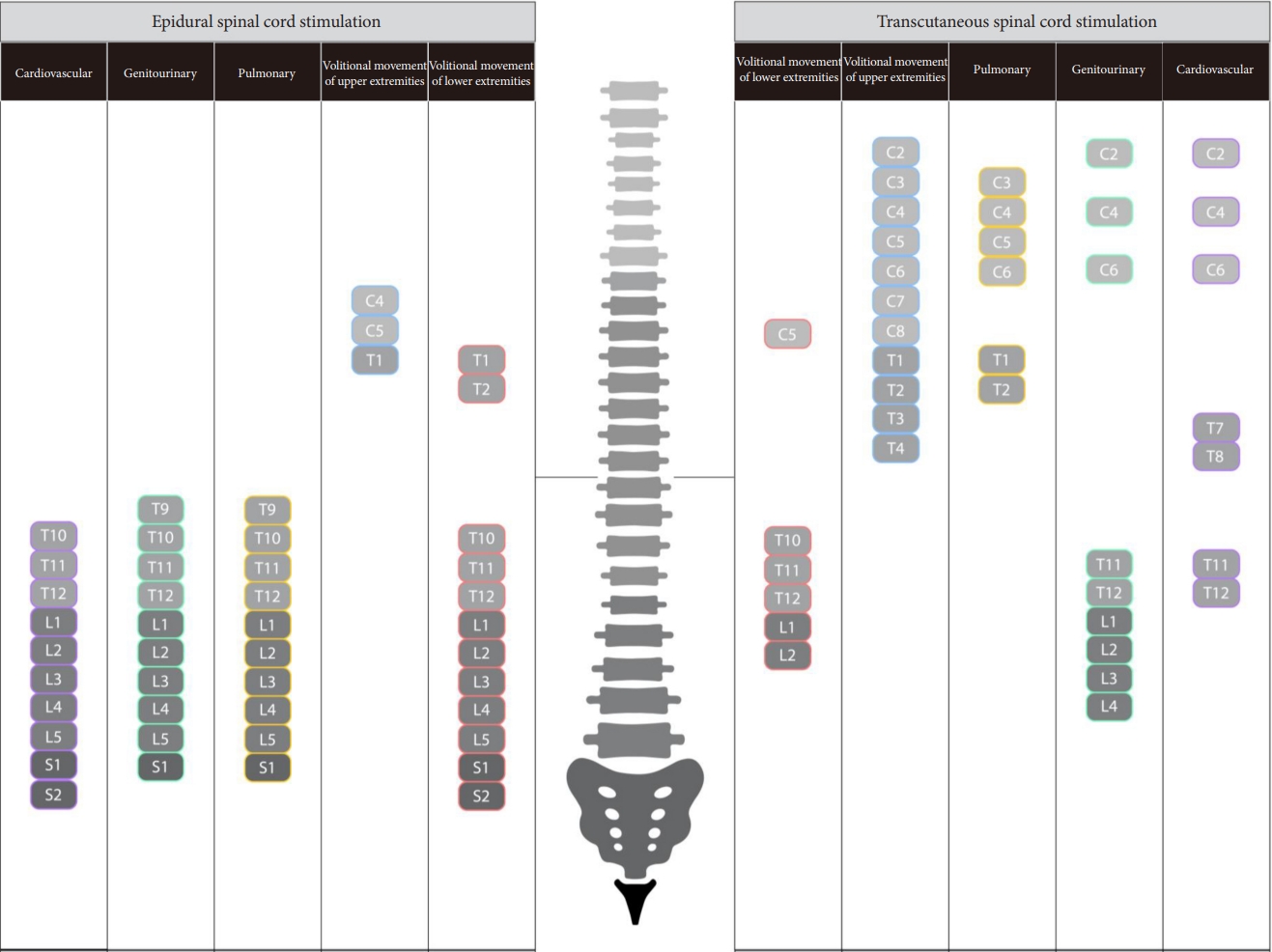
The main stimulation parameters of the eSCS studies are shown in Table 2. The main stimulation parameters of the tSCS studies are shown in Table 3. Of these studies, 48 used eSCS and 24 used tSCS. Of the studies using eSCS, most studies used a Medtronic stimulator (31 of 48) with 16-electrode paddle leads. The locations of lead placement for both eSCS and tSCS studies are shown in Fig. 2. The highest level of lead placement was C2 via tSCS reported by Inanici et al. [86]. The lowest level of lead placement was Co1 via tSCS by Gad et al. [40]. The most common and effective level of lead placement for volitional movement of lower extremities was in the range of T10ŌĆōL2. The most common and effective level of lead placement for volitional movement of upper extremities was in the range of C4ŌĆō6. For genitourinary function, the most common and effective level of lead placement was L1-S1. Lead placement for pulmonary function studies was most common and most effective at T9ŌĆō11. The most common level of lead placement for cardiovascular function was T11ŌĆōL1, which has been shown to be effective in reducing orthostatic hypotension [40,45,54,57,66,71,72]. However, lead placement at T7ŌĆō8 and L1ŌĆōS1 were also found to be effective for addressing cardiovascular function [50,58,76,86]. The range of stimulus locations can be seen in Fig. 2. Stimulation parameters varied across the studies. We categorized stimulation parameters into 2 major categories: tonic stimulation, where uniform pulses or pulse trains were fired, or spatiotemporal modulation, where spatially selective stimulation was optimized to induce intended movements. Only one study included spatiotemporal modulation of stimulation, though Rowald et al. (a study published outside of our search parameters) used spatiotemporal modulation as well [2,15]. Pulse widths ranged from 150 ╬╝sec to 2 msec. Current intensities ranged from 0.1ŌĆō15 mA/1ŌĆō40 V in eSCS studies and 2.5ŌĆō210 mA/18 V in tSCS studies, though most studies used high intensities close to the subjectsŌĆÖ tolerance threshold. The most common and most effective stimulation settings for lower extremity volitional movement were spatially directed based on settings optimized for individual patients performing specific activities (based on muscle group activation). Upper extremity volitional movement was most commonly studied using 0.5ŌĆō1.0 ms bursts of stimulation at 0.2ŌĆō90 Hz with carrier frequencies of 2.5ŌĆō10 kHz, which was found to be effective, though Lu et al. [38] found that spatially directed stimulation optimized for individual patients and activities were also effective. For genitourinary function, the most common stimulation settings were spatially directed and optimized for specific patients and specific activities but optimization for volitional activity of lower extremities was ineffective in improving genitourinary outcomes. Instead, tonic stimulation at 2ŌĆō60 Hz was effective in improving bladder storage and voiding. Stimulation settings for pulmonary function studies were most common and effective with tonic stimulation at 2ŌĆō60 Hz. The most common stimulation settings for cardiovascular function were spatially directed, an effective setting for improving cardiovascular outcomes.
The main outcomes of the eSCS studies are shown in Table 4. The main outcomes of the tSCS studies are shown in Table 5. Positive volitional outcomes were measured in terms of electromyography (EMG) activity consistent with activities such as stepping, gait analysis consistent with more fluid movements, increased muscle strength, achievement of independent sitting, increased body weight support, achievement of A/I step, achievement of A/I stand, increased fluidity of sit to stand transition, improved treadmill step/walk, improved overground walking, increased home and community access, increased walking speed, decreased spasticity, decreased sense of effort, or improved ASIA score. Positive genitourinary outcomes were measured in terms of EMG activity consistent with better muscle control, decreased incontinence, increased storage and voiding volume, decreased urinary complications, improved urodynamic parameters via cystometry, decreased time and effort used in bowel management, achievement of orgasm, and decreased Neurogenic Bladder Symptom Score. Positive cardiovascular outcomes were measured in terms of stable blood pressure, improved blood pressure regulation during orthostasis, improved cardiac function, stable heart rate, normal middle cerebral artery blood flow, increased metabolic rate, and increased oxygen consumption. Positive pulmonary outcomes were measured in terms of increased airway pressure, increased ability to cough, increased air flow rate, and decreased volume of respiratory secretions. All but one study reported positive outcomesŌĆöBeck et al. [62] reported worsening genitourinary function when using eSCS parameters optimized for volitional movement. Of the 51 studies examining sensorimotor function, 45 studies evaluated lower extremity function and 6 studies evaluated hand function. With regards to autonomic function, 10 studies examined genitourinary function, 8 studies examined pulmonary function, and 11 studies examined cardiovascular function. Four studies reported the return of volitional movement without stimulation [2,42,78,81]. Physical training was described preimplantation in 24 studies and postimplantation in 33 studies, though number of sessions ranged from none to 160 sessions and duration of sessions ranged from 0.5ŌĆō3 hours. Six studies reported the return of autonomic function during stimulation [50,59,74,76]. One study reported the experience of orgasm for the first time since injury in a patient [76]. Out of 327 patients with varying stimulation and evaluation protocols, 118/127 patients saw improvement in sensorimotor function during stimulation, 51 of 70 patients saw improvement in autonomic genitourinary function during stimulation, 32 of 32 patients saw improvement in autonomic pulmonary function during stimulation, and 32 of 36 patients saw improvement in autonomic cardiovascular function during stimulation. Most patients with improvements in sensorimotor function underwent extensive physical training, ranging from one month to almost 4 years. Of the 127 patients studied for changes in sensorimotor function, 8 patients did not see improvement in motor function, potentially due to lower spasticity scores prior to treatment [69,81]. Seventy-one of 127 patients saw return of volitional movement during stimulation. After months of physical training with adjunctive SCS, 7 of 127 patients saw lasting return of volitional movement in the absence of stimulation for months. In general, there was good tolerability of the intervention by patients with few significant complications.
DISCUSSION
The use of electricity to modulate the nervous system has existed throughout history with variable efficacy. Though use of electricity for neuromodulation has existed since the Ancient Egyptians, studies of electrical stimulation of the spinal cord began in the late 1900s [89,90]. Electrical stimulation of the spinal cord was first tested in 1967 when Norman Shealy applied electrical stimulation subdurally to the dorsal column of cats and found prolonged after-discharge upon electrical stimulation [90]. Based on these findings, Shealy partnered with a graduate engineering student, Thomas Mortimer, to develop an implantable spinal cord stimulator by modifying cardiovascular stimulators [91]. Subsequently, use of spinal electrical stimulation was applied in a human patient for temporary severe pain management [92]. More recent approaches to SCS for management of chronic pain include burst stimulation to deliver square waves (5 spikes at 40- Hz bursts with each burst at 500 Hz) or high frequency stimulation (10 kHz) via the Senza system [93,94]. Although the exact mechanism of pain relief during SCS remains unclear, the Gate Control Theory has prevailed as the main explanation for decreased pain perception with stimulation. As hypothesized by the Gate Control Theory, the analgesic effects of SCS are achieved due to greater sensory information being carried by large diameter (touch, vibration, pressure) fibers relative to sensory information being carried by small diameter (pain) fibers to the dorsal horn of the spinal cord [95]. SCS has improved over time, first with the transition of electrode placement from subdural to epidural, then with technological advancements allowing for fully implanted systems with battery-powered pulse generators [96,97]. These advancements have led to further mechanistic rodent studies on the effect of SCS on functional recovery following SCI, such as return of motor, sensory, or autonomic function below the injury site [16].
The mechanism of action for return of function with SCS after SCI is not fully understood, though current mouse models suggest that SCS transforms dormant tissue to active tissue at the injury site by increasing general excitability [16]. Central pattern generators (CPGs) are dedicated spinal circuits that elicit coordinated rhythmic activity of multiple musclesŌĆöCPGs also control reflex influences on alpha motor neurons by facilitating or inhibiting these neurons during specific phases of motion [98]. In rats, stimulation of CPGs in a regular pattern, with the fixed time periods between each stimulation, has been shown to induce adaptive plasticity, promoting spinal cord learning, whereas unsynchronized stimulation has been shown to generate maladaptive spinal plasticity, increasing nociceptive hyperreactivity [99,100]. Coupled with extensive physical training, modulation of excitability allows sensory information to be used as a source of control for voluntary movement through appropriate remodeling of supraspinal and intraspinal pathways in mouse models [16]. However, it should be noted that there are notable anatomical differences between rodents, larger animal models, and humans. For example, rhesus monkeys are more comparable to humans in the projection of the corticospinal tracts. In primates, the corticospinal tract projects through the dorsolateral column, and contains axons originating from both the left and right motor cortex. In contrast, in rodents the corticospinal tract is primarily located in the dorsal column, and these axons exclusively originate from the contralateral motor cortex. A substantial number of corticospinal axons decussate along the spinal cord midline in monkeys, but not in rodents [101]. These anatomical considerations should be taken into account when comparing mechanistic studies with clinical outcomes.
The majority of the functional improvements shown with SCS have been paired with periods of intense motor training. On average, 5.4 months of physical training was required for improvements in volitional movement, such as EMG activity consistent with step-like activity, gait analysis consistent with more fluid movements, increased muscle strength or improved ASIA scoreŌĆömost patients did not completely regain volitional movement. Innovations in approach, such as spatiotemporally modulated dorsal root targeted stimulation, enables activity-based movement within 1 day of stimulation [15]. By pairing stimulation and physical training, plastic changes can be achieved, leading to return of volitional movement in the absence of stimulation. On average, 6.48 months of physical training was required for return of volitional movement in the absence of stimulation in patientsŌĆöAlam et al. [78] demonstrated the return of volitional movement in the absence of stimulation after 3 months of physical training whereas Rejc et al. [42] demonstrated return of volitional movement in the absence of stimulation after 5.5 years of physical training including 21 months of training prior to stimulator implantation. The remodeling of supraspinal and intraspinal pathways of these patients likely occurs using the same mechanisms underlying learning and memory in the hippocampusŌĆöin response to stimulation, AMPA (╬▒-amino-3-hydroxy-5-methyl-4-isoxazoleproprionic acid) and NMDA (N-methyl-D-aspartate) receptors mediate long-term potentiation and long-term depression [102]. Current studies using electricity to treat chronic SCI in rodent models as well as human patients show that electricity is an efficacious neuromodulator for recovery from SCI when paired with physical training, but the optimal amount of training is likely subject dependent and requires further study.
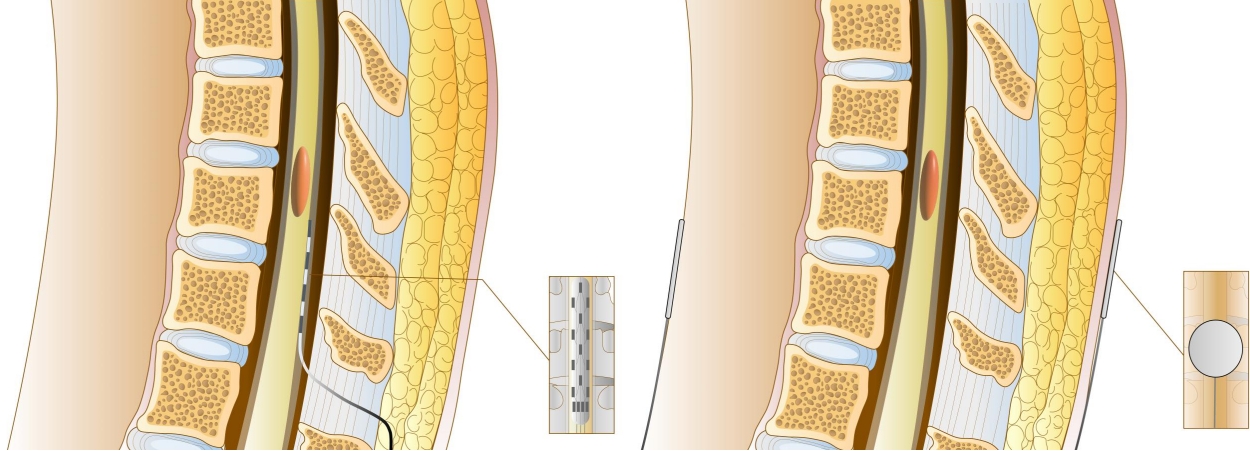
Recently, eSCS and tSCS have both emerged as electricity-based neuromodulation that target the spinal cord, and have shown impressive results in the restoration of function in individuals with SCI. eSCS is defined by the delivery of electricity to the dorsal surface of the dura mater of the spinal cord [103]. Though most commonly used for chronic pain management, eSCS has been shown to improve motor strength and voluntary motor function in patients with SCI [28,104]. tSCS, much like eSCS, elicits spinal cord reflex activity but has electrodes placed on the skin instead of on the dura [30,105]. Through utilizing unique waveforms, tSCS permits high-current electrical stimulation to reach spinal networks without causing discomfort [34]. The differences in electrode placement between epidural SCS and tSCS in stimulation location are visualized in Fig. 3. Both techniques activate the dorsal roots, though tSCS stimulation of the skin may contribute to elevated neural activity as well [73,106]. The dorsal roots are comprised of primary afferent fibersŌĆöthese large diameter proprioceptive sensory fibers have the lowest activation threshold and are preferentially recruited during stimulation [107]. eSCS produces a localized electric field resulting in higher segmental selectivity of the recruited dorsal roots, a feature that allows induction of nonvolitional movements [24,27]. tSCS produces a more distant and unfocused electric field with less segmental selectivityŌĆöby providing uniform bilateral coverage of several spinal cord segments, tSCS can increase the general excitability of the spinal cord to induce volitional movement in conjunction with physical training [35,39,108]. Though eSCS and tSCS differ in application, both have been shown to be efficacious in eliciting functional recovery following SCI, and further research should be performed to compare and contrast outcomes with these techniques.
1. Sensorimotor Function
Both eSCS and tSCS have been shown to restore sensorimotor function, most notably measured in return of volitional movement and changes in EMG activity. Of the 127 patients studied for sensorimotor function, 71 patients regained volitional movement during SCS, 51 using eSCS and 20 using tSCS. Of the 51 patients to regain volitional movement during eSCS, 28 patients were noted to have complete SCI (ASIA A) and 23 patients were noted to have incomplete SCI. Of the 20 patients to regain volitional movement during tSCS, none were noted to have complete SCI (ASIA A) and 19 patients were noted to have incomplete SCI, with one patientŌĆÖs SCI injury grade not reported. Usage of eSCS in conjunction with months of physical training induced return of volitional movement without eSCS in 7 patients [2,42,81]. Usage of tonic tSCS at T11 and L1 in conjunction with extensive physical training also induced return of volitional leg movements without stimulation in a single patient, as well as increased pin-point sensation [78]. These studies examine volitional movement, which requires a descending depolarizing input to reach motor threshold, activating motor neurons involved in movement [109]. Immediate improvements in muscle strength and sensation may be explained by modulation of spinal networks into a physiologic state that enables greater access of supraspinal control to sensorimotor networks [73]. In individuals with complete SCI, stimulation is postulated to access local spinal circuitry via dorsal root primary afferent fibers [107,110]. For individuals with an incomplete SCI, SCS is postulated to increase the descending activation of spinal inhibitory circuitry through brainstem-spinal cord loops (orthodromic conduction), as well as activating dorsal column fibers to modulate activity of segmental circuitry involved in regulation of afferent inputs and motor neuron excitability (antidromic conduction) [111,112]. The tonic activation of the dorsal root afferent fibers elevates spinal network excitability and brings both interneurons and motor neurons closer to motor threshold, making the circuit more likely to respond to limited post-injury descending drive [12,113,114]. Recent preclinical and clinical studies have examined the usage of SCS with targeted spatiotemporal eSCS to activate discrete sensorimotor networks during locomotion and other pattern-based activities [2,115,116]. By developing software to support rapid configuration of stimulation programs that reproduced natural activity-specific activation of motor neurons, Rowald et al. [15] were able to use spatiotemporally modulated eSCS on SCI patients to enable activity-dependent movements such as walking and cycling. Due to the heterogeneity of SCI and differences in spinal anatomy, intensive stimulation optimization or computational modeling for individual subjects may be necessary to increase the efficacy of spatiotemporal stimulation. The studies reviewed show great potential for therapeutic applications of eSCS in restoring motor function in patients with severe SCI, especially with optimized and targeted approaches.
2. Genitourinary Function
Both eSCS at T11ŌĆōL1 and L1ŌĆōS2 and tSCS at T11ŌĆōL3/L4 have been shown to improve bowel-bladder function in patients with SCI. Usage of spatially directed eSCS, specifically on the caudal end of a T11ŌĆōL1 array or on the rostral end of a L1ŌĆōS2 array, improved bowel-bladder function [53,76]. Stimulation using the caudal end of a T11ŌĆōL1 array (pulse width of 390ŌĆō450 ╬╝sec, frequency 25ŌĆō45 Hz, intensity 4ŌĆō7 V) in a young male patient (32 years old) 5 years after sustaining motor complete, sensory incomplete SCI increased external anal sphincter/pelvic floor muscle tone and detrusor pressureŌĆöthese effects significantly expedited bowel management (p= 0.039) and decreased the severity of neurogenic bowel dysfunction from severe to minor, as seen in a reduction in neurogenic bowel dysfunction score from 15 to 8 and improvement of general satisfaction scale from 5 to 8 [53]. Stimulation using the rostral end of an L1ŌĆōS2 electrode to excite caudal preganglionic neurons distributed between T1 and L2 in two older female patients in their fifth and sixth decade of life, five and 10 years after sustaining motor and sensory-complete SCI, allowed improvement of bowel-bladder synergy in both patients but recovery of ability to void volitionally but incompletely with residual volumes in only one patients [76]. Conversely, usage of tonic tSCS to stimulate T11ŌĆōL3/4 at 1Hz improved bladder function during stimulation in 5/5 patients, increasing the volume of urine produced voluntarily from none to 1,120 mL/day, decreasing the frequency of self-catheterization from 6.6/day to 2.4/day, and increasing bladder capacity from 244 mL to 404 mL [74]. SCS is currently hypothesized to enable genitourinary function via an increase in storage and voiding reflexes as well as volitional sphincter control by allowing the micturition circuitry in the sacral cord to appropriately respond to residual descending input from supraspinal micturition centers [74]. Taken together, these studies indicate that SCS of preganglionic neurons near L1 is safe and effective in improving bowel-bladder function in chronic SCI patients.
3. Pulmonary Function
Both eSCS and tSCS have been used to improve pulmonary function in patients with SCI. Regular use of tonic eSCS at T9ŌĆōL1 (40 V, 30ŌĆō55 Hz) can lead to pulmonary function changes, notably an increase over 10 and 20 weeks in positive expiratory pressure generation to restore cough [26,46,59]. Additionally, usage of tonic tSCS with a 10-kHz carrier pulse and a 30-Hz burst pulse at the C3ŌĆō4, C5ŌĆō6, and T1ŌĆō12 improved breathing and coughing ability in a patient, with improvements persisting for a few days after tSCS was stopped [60]. Pulmonary function changes in response to SCS are likely due to induction of an excitatory functional state leading to recruitment of respiratory intercostal and trunk muscles [60]. Additionally, dorsal lower thoracic SCS may lead to activation of spinal cord pathways with connections to phrenic motor neuron pools, leading to coactivation of the diaphragm as well [117]. Both eSCS and tSCS hold promise in improving pulmonary function for patients with SCI, though further study of the effects of tSCS are necessary to confirm these findings.
4. Cardiovascular Function
eSCS and tSCS has been demonstrated to restore autonomic cardiovascular function in patients with SCI. Phillips et al. [50] reported return of autonomic cardiovascular function during an orthostatic challenge, noting normalization of blood pressure and heart rate, with tonic monophasic tSCS at 30 Hz at the T7 level. Similar results as discussed with tSCS have been shown with eSCS as well, noting resolution of orthostatic hypotension [54,118]. Cardiovascular function changes in response to SCS, as measured by normalization of heart rate or blood pressure, are likely due to 2 possible mechanisms involving sympathetic preganglionic neuron excitation: (1) small caliber C-fiber afferents excitation, leading to propriospinal interneuron overactivity associated with autonomic dysreflexia, or (2) propriospinal and sympathetic preganglionic neurons excitation, either directly through electrical stimulation or by preferential excitation of large diameter sensory axons that do not elicit autonomic dysreflexia [50,66]. As orthostatic hypotension can have a large negative effect on quality of life, further study of the effects of tSCS and eSCS, on cardiovascular function is necessary.
5. Risk of Bias
A detailed list of risk of bias assessments using ROBINS-I is provided in Supplementary Table 1. Within each study, the risk of bias was judged overall as serious for 66 publications. The bias in measurement of outcomes was the primary source of bias due to lack of blinding in the majority of studies. Additionally, though most studies included patients acting as their own controls with ŌĆ£stimulator onŌĆØ versus ŌĆ£stimulator offŌĆØ settings, many patients themselves reported being able to discern between on and off states of the stimulator, and therefore cannot be reliably blinded. The judgement of risk of preintervention domains (confounding, selection, and classification biases) ranged from moderate to serious, where moderate was the lowest possible risk of bias for intervention studies. Most studies were considered low risk for deviation from intended interventions (n= 53) and low risk for missing data (n= 65). Studies ranged from low to moderate with regards to risk of bias for selective reporting.
6. Safety of SCS
SCS is well-documented as a safe treatment for chronic pain due to its reversible and minimally invasive characteristics [119]. Catastrophic complications, such as life-threatening infections or new neurological deficits, are incredibly rare, noting only one reported case of death due to infection and one reported case of paralysis from epidural abscess prior to 2007 [120]. The incidence of minor complications with SCS has been reported to be around 30%ŌĆō40%, though these minor complications occur within 12 months of implantation and are generally resolved [121]. Complications of mechanical origin (rate of 24%ŌĆō50%), such as lead fracture or disconnection (rate of 5%ŌĆō9%), lead migration (rate of 0%ŌĆō27%), or implantable pulse generator failure (rate of 1.7%), are far more common than complications of biological origin (rate of 7.5%), including events like infection (rate of 3%ŌĆō8%) or dural puncture (rate of 0.3%ŌĆō2%) [119,122,123]. However, the possibility of adverse events in the use of SCS in patients with SCI, particularly with regards to infection, needs further study. Though not present in the studies listed above, there have been a number of patients with surgical site infections after epidural SCS placement [124]. The results of this review indicate that both epidural and transcutaneous SCS are viable options for increasing voluntary motor response of the upper and lower limbs, trunk stability, and autonomic function in patients with SCI. The limited number of complications suggest that both forms of SCS are safe and well tolerated. Both epidural and transcutaneous SCS had cases of dermatologic issues that resolved with time. The 2 reports of potential autonomic dysreflexia self-resolved, one caused by epidural SCS and the other by transcutaneous SCS. Across the studies listed above, there was a 4% complication rate, noting 5 potential cases of autonomic dysreflexia, 3 cases of skin breakage or infection, 1 case of mild drainage from the surgery site, 1 case of a mild skin allergy, 2 cases of a single nonfunctional lead, and 1 case of ankle edema. Stimulation parameters were adjusted to lower levels of patient discomfort, though discomfort at increased frequencies of stimulation (~100 Hz) was more prevalent with epidural SCS.
While research has shown using SCS is a safe and effective option in treating patients with SCI, many steps are necessary for SCS to become a standard treatment for return of motor and autonomic function in SCI patients. The number of clinical trials examining SCS use in SCI has increased over the past 5 years, especially with regards to volitional and nonvolitional movement. A search of ongoing clinical trials pertaining to SCS use in SCI patients was conducted using the publicly available trial registry, ClinicalTrials.gov (https://clinicaltrials.gov/). This search was conducted on March 12th, 2022 and included the search terms ŌĆ£spinal cord injuryŌĆØ and ŌĆ£spinal cord stimulation.ŌĆØ After screening for trials specifically using eSCS or tSCS, 60 active trials were identified, with 23 studies using eSCS, 35 studies using tSCS, and 2 studies using eSCS as well as tSCS. 4 studies are currently examining the use of SCS on children with SCI. Forty studies are examining SCS effects on sensorimotor function (both volitional and nonvolitional), 7 studies are examining effects of SCS on autonomic cardiovascular function, 9 studies are examining effects of SCS on pulmonary function, and 9 studies are examining effects of SCS on the genitourinary system. Additionally, 3 studies are examining effects of SCS on muscle electrical activity and 4 studies are examining effects of SCS on muscle spasticity. Additionally, many new clinical trials are studying different stimulation parameters as well as concurrent pharmacologic treatments. To move towards further clinical translation, further clinical trials should adopt more robust research designs to reduce bias, such as including control groups, incorporating randomization before implantation, and adding further blinding to patients and assessors, as well as developing the framework for multicenter studies in an effort to include more patients and make data accessible for external analysis [125].
The use of SCS to induce functional recovery after SCI is still a fairly new techniqueŌĆöthe data gathered across the studies listed in this paper are mostly from case or case-series studies with no appropriate control groups to assess if SCS is a better treatment than placebo or the current standard of care. The patients in the reviewed studies were mostly male (n= 257), indicating a gender biasŌĆöthough males are more commonly injured, these results suggest that more females should be included in SCS studies to identify potential gender differences. Additionally, age ranged from 18 to 66 years, but the age recommended for implantation may differ based on the indication for SCS [126,127]. Time between injury and enrollment ranged from 0.1 to 41.1 years, indicating that delayed implantation was not contraindicated. The patients studied had a wide range of injury levels, demonstrating the effectiveness of SCS in treating diverse patient populations, but making it difficult to draw conclusions on the most suitable patient population for SCS. Our review of the literature reveals that further standardization of optimal stimulation frequency and location to elicit specific outcomes, such as bladder control or autonomic cardiovascular response, are necessary. Currently, stimulators used in SCS are designed for chronic pain treatment rather than return of sensorimotor or autonomic functionŌĆö given that the optimal stimulation parameters differ greatly both between individuals and between specific functions, both sensorimotor and autonomic, stimulators with greater programmability would be greatly beneficial for further studies. Given rat model data has shown that SCS amplifies pre-existing signals in the remaining intact tissue after SCI, individuals with anatomically intact tissue at the injury site may be good candidates for treatment [4]. However, further research needs to be done to assess which subjects will respond most efficaciously to neuromodulation therapy, and whether eSCS or tSCS will be of greatest utility for each individual.
CONCLUSION
The results of this review indicate that epidural and transcutaneous spinal cord stimulation are active areas of study holding promise for improving motor and autonomic function following SCI. Although the results of these studies are positive, significant research still needs to be performed to transition the use of SCS in the restoration of function following SCI from basic research to clinical use. Further mechanistic studies are needed to define optimal stimulation parameters and develop a greater understanding of how SCS interacts with residual connections across the SCI lesion. Based on the current reported results, it is likely that restoration of different functions require optimization by delivering stimulation at distinct spinal levels and with specific parameters. Additionally, structured clinical trials with increased number of subjects need to be performed to evaluate the parameters necessary for greatest efficacy in eSCS and tSCS treatment of patients with chronic SCI.










")













