







INTRODUCTION
Traumatic cervical spinal cord injury (TCSCI) is a devastating disease that leads to lifelong disability and long-term risk of medical complications [1-3]. TCSCI often results in acute respiratory failure [4]. Many researchers have demonstrated that early tracheostomy (≤ 7 days from intubation) can bring many benefits to patients with TCSCI [4-7]. For example, early tracheostomy may reduce mechanical ventilation (MV) time and allow for more comfortable and efficient breathing. To take advantage of these benefits and allocate resources accordingly, it is important for surgeons to have a tool to predict whether a patient might need a tracheostomy.
Although several factors for tracheostomy have been identified through multivariate logistic regression analysis (MLRA) and classification and regression tree (CART) model [8-11], early prediction of tracheostomy in TCSCI patients is still difficult. The nomogram is an essential part of modern medicine and is considered a reliable and practical predictive tool [12,13]. The nomogram can visually display the results of MLRA, and can also predict the probability through a simple picture representation [14-16]. To the best of our knowledge, no nomogram prediction model of tracheostomy has been reported in TCSCI patients. The purpose of this study was to develop and validate a simple and convenient nomogram model for predicting tracheostomy after TCSCI.
MATERIALS AND METHODS
1. Study Design
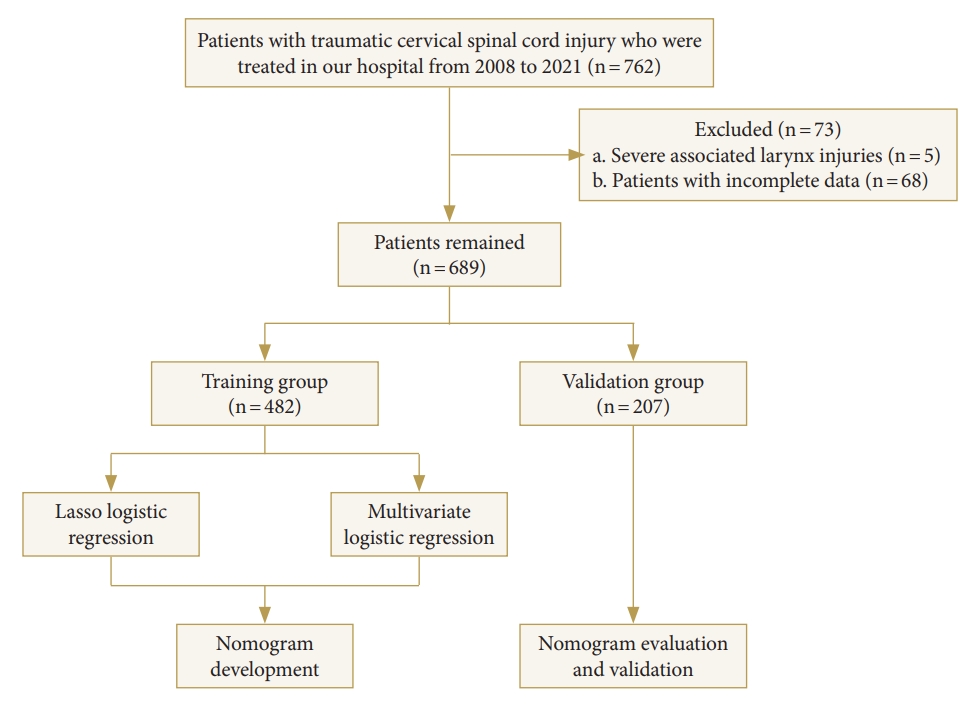
This was a retrospective study. This study was based on data from a university hospital in Chongqing, China between January 2008 to December 2021. It was approved by the Ethics Committee of our hospital. TCSCI was diagnosed by taking into account a history of trauma, symptoms, consciousness, sensory and motor, complete neurological testing, and imaging findings such as computed tomography and/or magnetic resonance imaging [17]. The decision to perform a tracheostomy was made by the spine surgeon in conjunction with the intensive care unit physician and was made when prolongation of the MV was expected, considering the patient’s neurologic function, respiratory function, age, concomitant injury, and other factors. Tracheostomy was performed if any of the following criteria were met: (1) the patient was retained in a transoral tracheal tube and failed to evacuate MV after several attempts; (2) the patient had a lot of sputum and poor coughing power, requiring retention of an artificial airway to drain sputum. All assessments were performed by experienced senior physicians on admission. The overall flow chart is shown in Fig. 1.
2. Study Participants
A total of 762 patients with TCSCI in the department of orthopedics were analyzed. The inclusion criteria were as follows: (1) clear history of trauma, (2) well-diagnosed cervical spinal cord injury, and (3) complete medical records. The exclusion criteria were as follows: (1) larynx injuries, (2) patients who underwent tracheostomy at other hospital, and (3) incomplete medical records. Finally, 689 patients were included in the study sample.
3. Data Collection
The relevant patient’s data were recorded, including sex, age, smoking history, dislocation, diabetes mellitus, hypertension, preexisting lung disease, brain injury, American Spinal Injury Association (ASIA) impairment scale grade, neurological level of injury (NLI), and thoracic injury. ASIA impairment scale grade was assessed using the ASIA standards [18]. ASIA impairment scale grade was divided into grades A and B–D. NLI was divided into C1–4 and C5–8. The dislocation was defined as traumatic cervical facet dislocation confirmed by radiological examination. Preexisting lung diseases included chronic obstructive pulmonary disease, bronchial asthma, and restrictive lung disease. According to World Health Organization, smoking was defined as continuous or cumulative smoking for 6 months or more in a lifetime [19].
4. Statistical Analysis
All patients were randomized into training and validation groups, in a 7:3 ratio for nomogram construction and validation. Pearson chi-square test and LASSO regression analysis were used to screen variables. The screened variables were brought into MLRA in a step-by-step method to determine the independent predictors. Based on the MLRA, a nomogram prediction model of tracheostomy was constructed. The area under curve (AUC) was calculated in training and validation groups to measure the predictive accuracy of the nomogram model. The calibration curve and Hosmer-Lemeshow test were performed to assess the predictive ability of the nomogram. The decision curve analysis (DCA) was performed to evaluate the predictive model. All analyses and nomogram development were performed using R ver. 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). A p-value of < 0.05 was considered statistically significant.
RESULTS
1. Baseline Characteristics in Training Group
In the training group, 482 patients with TCSCI, and 74 patients (15.4%) underwent tracheostomy. The baseline characteristics of patients in the training group are shown in Table 1. A comparison of patients with and without tracheostomy is shown in Table 2. Compared with the nontracheostomy group, the tracheostomy group presents a significant difference in age ≥ 60 years, sex, smoking history, dislocation, ASIA impairment scale, NLI, and thoracic injury (p < 0.05).
2. LASSO Regression and MLRA
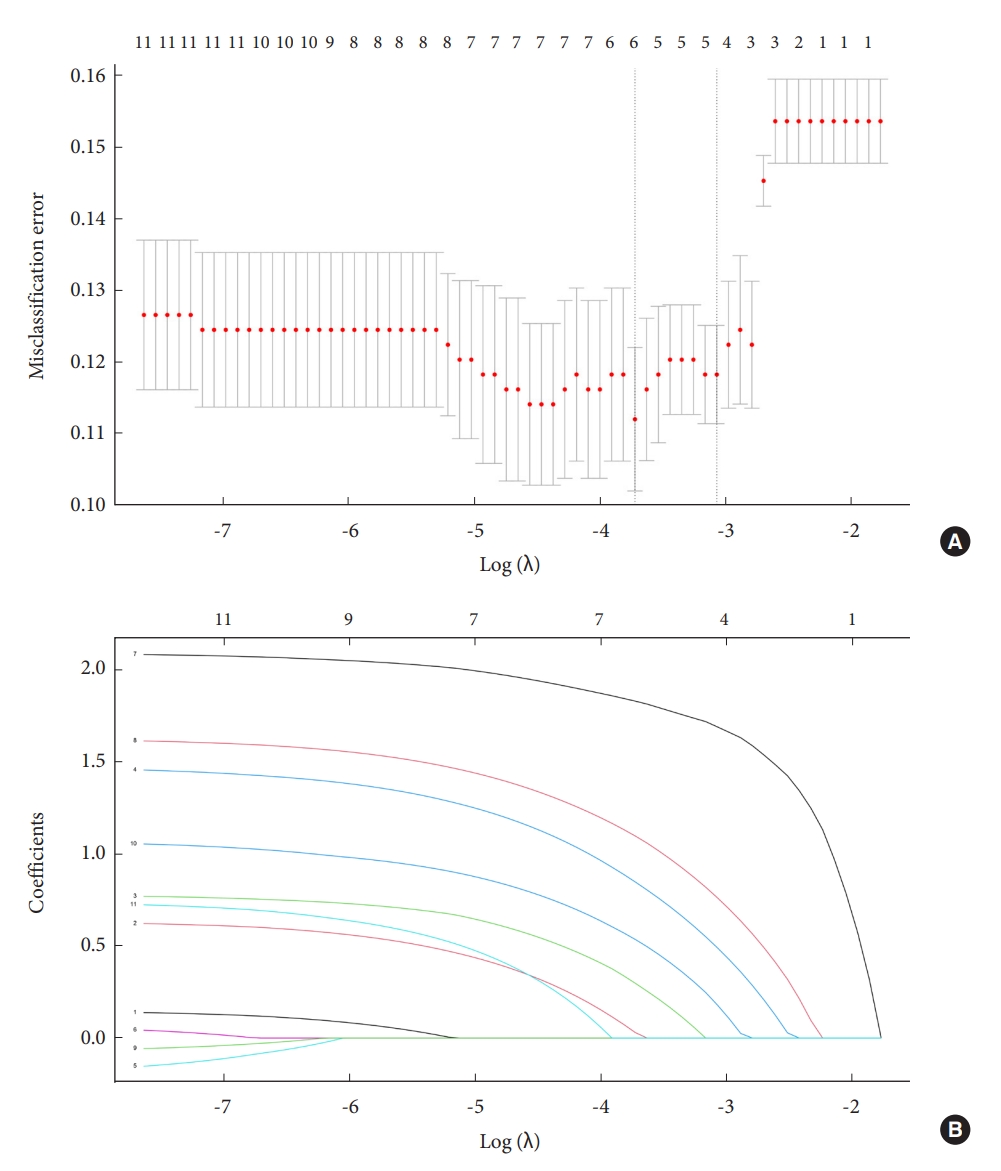
The variables screened by LASSO regression analysis were: age, smoking history, dislocation, ASIA impairment scale grade, NLI, and thoracic injury (Fig. 2A, B). Their optimal coefficients were 0.029, 0.297, 0.847, 1.830, 1.097, and 0.535, respectively. These 6 variables selected by the LASSO regression with nonzero coefficients were included in the MLRA analysis. The results of the MLRA are given in Table 3. Five variables, including smoking history, dislocation, thoracic injury, ASIA impairment scale grade, and NLI, showed significant statistical differences.
3. Nomogram Model Development
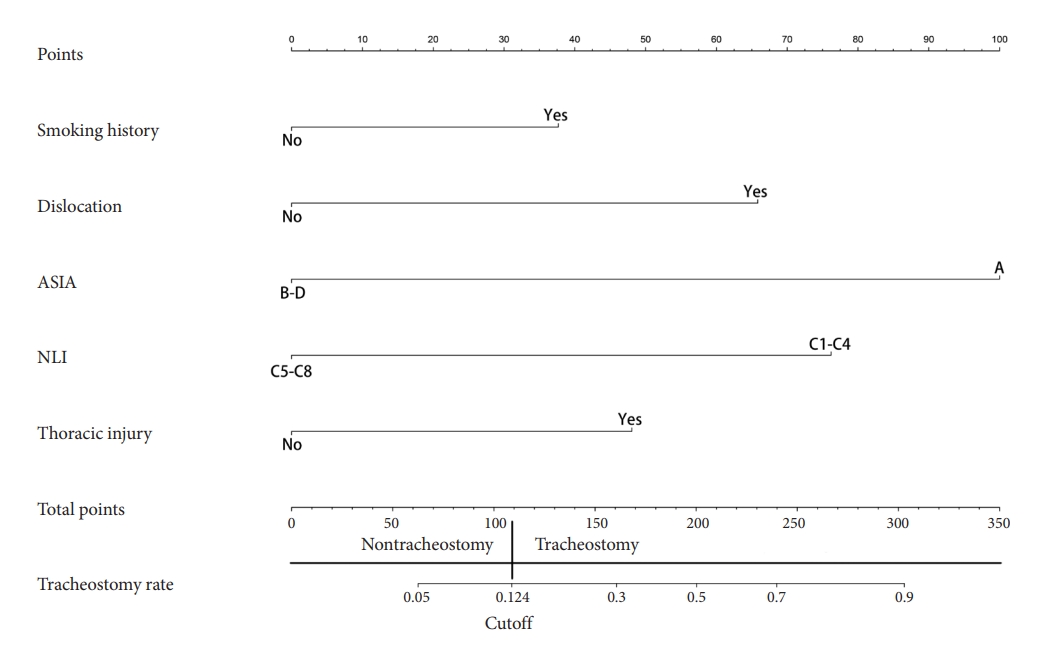
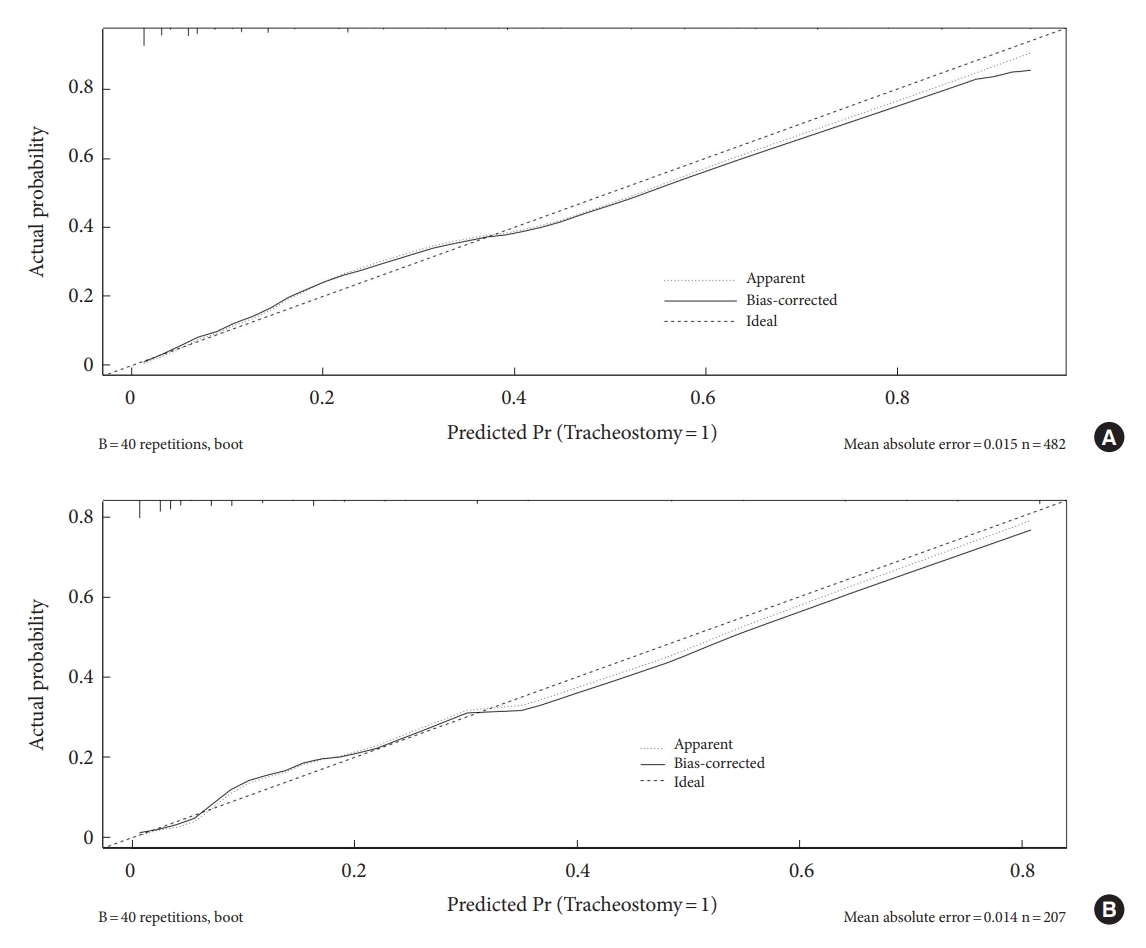
Using these 5 variables, a nomogram model for predicting tracheostomy was developed (Fig. 3). Each factor corresponded to a score at the top of the nomogram, and the total score was calculated and compared to the bottom of the nomogram to predict tracheostomy risk. The AUC in the training group was 0.883. The best cutoff point was 0.124 (sensitivity, 0.838; specificity, 0.770) (Fig. 4A), which indicated that the discrimination of the nomogram model was good. The calibration curve of the nomogram model revealed satisfactory consistency (Fig. 5A).
4. Validation With Validation Set
Twenty-eight patients (13.5%) in the validation group underwent tracheostomy. The result of the Hosmer-Lemeshow test was p = 0.153. The AUC in the validation group was 0.909. The best cutoff point was 0.136 (sensitivity, 0.893; specificity, 0.777) (Fig. 4B), which indicated that the discrimination of the nomogram model was good. The calibration curve of the nomogram model revealed satisfactory consistency in the validation group (Fig. 5B).
DISCUSSION
The study presented 102 of 689 TCSCI patients who underwent tracheostomy to comprehensively screen the independent risk factors. In the MLRA analysis, dislocation, thoracic injury, ASIA grade A, NLI, and smoking history were associated with tracheostomy in TCSCI patients. Based on these results, a nomogram model was developed. Then, the model was validated on the training set and validation set. This nomogram model showed that dislocation, thoracic injury, ASIA grade A, NLI at C1–4, and smoking history were key predictors. This study provided a relatively reliable nomogram model. It exhibited relatively good discrimination and calibration capabilities.
The ASIA grade A has been regarded as an essential predictor for tracheostomy in TCSCI patients [10,20-26]. It was also an important predictor in the CART model for predicting tracheostomy [8]. In the results of Childs et al. [27], they even suggested early tracheostomy in all patients with ASIA A. Consistent with previous research, the present MLRA results revealed that the ASIA grade A was a significant predictor of tracheostomy. In this nomogram prediction model, the score corresponding to ASIA grade A was the highest.
Due to diaphragm and/or intercostal muscle dysfunction, NLI was considered to be another important predictor for tracheostomy in TCSCI patients [25,28-31]. Tanaka et al. [32] suggested that tracheostomy may be required in patients with NLI C4 or above. The present study also classified NLI into C1–4 and C5–8. Consistent with previous studies, the score corresponding to NLI at C1–4 were also high in our nomogram prediction model.
This predictive model also included dislocation, smoking history, and thoracic injury. Cervical dislocations mostly cause spinal cord compression and dramatic neurological deficits. Mu et al. [26] also found that facet dislocation was a significant risk factor for tracheostomy in patients with TCSCI. Smoking increases susceptibility to pulmonary infection and the development of cigarette smoke-induced lung diseases [33]. Similarly, Nakashima et al. [11] found that one of the risk factors for tracheostomy was smoking history. One intriguing finding of the study was that thoracic injury was a predictor of tracheostomy. In the nomogram prediction model, thoracic injury corresponds to a score roughly around 50, between smoking history and dislocation.
Several risk variables associated with tracheostomy were presented in other studies, but not included in the present study. Some authors found that age was a statistically significant risk factor and that older age groups were more likely to undergo tracheostomy [10,21,26,34,35]. Controversially, other authors argued that age is not a risk factor [8,11,20,22,24,25,32]. Some scholars have introduced the forced vital capacity (FVC) variable in their prediction models [9,10]. However, using FVC for the predicted predictions has some shortcomings. For example, those who suffer great injury had to receive a tracheostomy may not have acceptable and reproducible pulmonary function test results [8,36].
There are 3 limitations to this study. First, this study was based on retrospective data from a single-specialty spine injury center, so the level of evidence is limited. Second, indications for tracheostomy in patients with TCSCI varied between institutions. Third, although the population was relatively large, the patients were from a single hospital. So, representation needs to be further improved.
CONCLUSION
The present study developed and validated a nomogram model that can predict tracheostomy in TCSCI patients. The nomogram combining dislocation, thoracic injury, ASIA grade A, NLI, and smoking history was validated as a reliable model for tracheostomy prediction. The present nomogram prediction model can help clinicians take timely and more targeted medical interventions.












")













