INTRODUCTION
Cavernous malformations (CMs) are rare vascular malformations with an incidence of about 0.4%–0.6% when occurring within the central nervous system [1,2]. Most of these benign lesions are usually intracranially located, particularly in the supratentorial compartment. Compared with their intracranial counterparts, only 3%–5% are in the spinal cord, with intramedullary spinal cavernous malformations (ISCMs) accounting for approximately 5%–12% of all spinal cord vascular disease [3-5]. With a considerably increased risk of hemorrhage or rehemorrhage events in CMs of the spinal cord compared to cerebral CMs, it is often associated with severe neurological deficits such as tetraplegia [6].
With the widespread use of magnetic resonance imaging (MRI), the detection rate of ISCMs has been rising [7,8]. Some ISCMs were found incidentally without symptoms, while others with chronic presentation or even acute onset of neurological deterioration. The natural course of ISCMs remains unclear, and the choice of conservative and surgical management remains controversial [9]. In the present study, we reported a consecutive case of 29 ISCMs patients in a single center, which was purely comprised of symptomatic patients who underwent microsurgical treatment. We reviewed and analyzed the clinical characteristics and surgical outcomes particularly focused on the risk for hemorrhage events and factors associated with neurological prognosis.
MATERIALS AND METHODS
1. Study Population
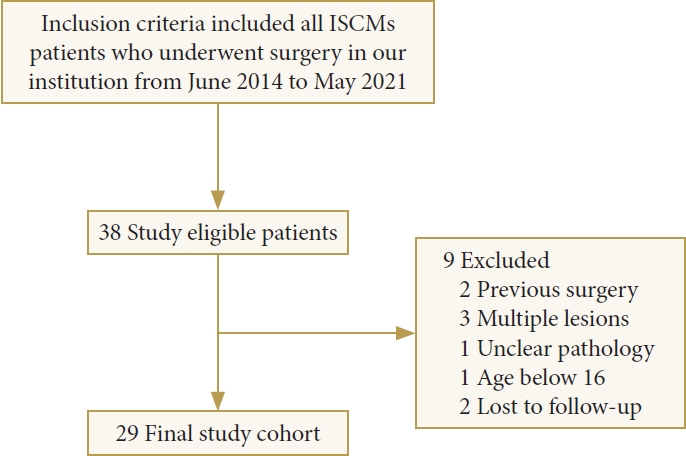
Twenty-nine consecutive patients with symptomatic ISCMs underwent surgical resection in the Neurosurgery department of Changzheng Hospital, Shanghai Institute of Neurosurgery, Shanghai, China, from June 2014 to May 2021 were retrospectively analyzed. The exclusion criteria included patients with previous microsurgical treatment, multiple lesions, unclear pathological diagnosis, and ages less than 16 years old. The patient’s medical records were reviewed for clinical symptoms, neuroimaging characteristics, intraoperative reports, surgical outcomes, pathology reports, and neurological progress. The study was approved by the Ethics Committee of Changzheng Hospital (No. 2022NS017), affiliated with Second Military Medical University (Shanghai, China), and written informed consent was obtained from each patient.
2. Data and Outcome Definition
Patient clinical data such as age, sex, clinical symptoms, location and lesion size, prior history of ISCM-related hemorrhage, postoperative status, etc., were properly collected. Patients’ preand postoperative neurological status was classified according to the modified McCormick scale (MMcS) [10,11] (Table 1). Clinical course before the presentation was classified into 3 types as described by Choi et al. [12]: acute onset of symptoms with the rapid decline (type A), slow progression of neurological degeneration (type C), or acute neurological deficit because of sequela from multiple previous hemorrhagic events (type M). MRI was performed preoperatively in all patients. The lesion size was defined as the maximum metric value to eliminate hemorrhage on the MRI inspection image. The annual retrospective hemorrhage rate was calculated using formula: hemorrhage rate= the number of hemorrhagic events/summation of patient age in years. A hemorrhage event was described as symptomatic with radiographic evidence of overt hemorrhage [13]. Intramedullary hemorrhage was defined as centrally and eccentrically located linear or flame-shaped nonedematous signal abnormality extending longitudinally away from SCMs, distinct from lesion rim [14].
The pathological diagnosis was confirmed postoperatively by 2 experienced pathologists independently. The ISCM-related hemorrhage was defined as an exacerbation of neurological deficits, MRI confirmation, and intraoperative findings. The extent of resection was defined as gross total resection (GTR), subtotal resection (STR), or partial resection.
3. Surgical Procedure and Follow-up
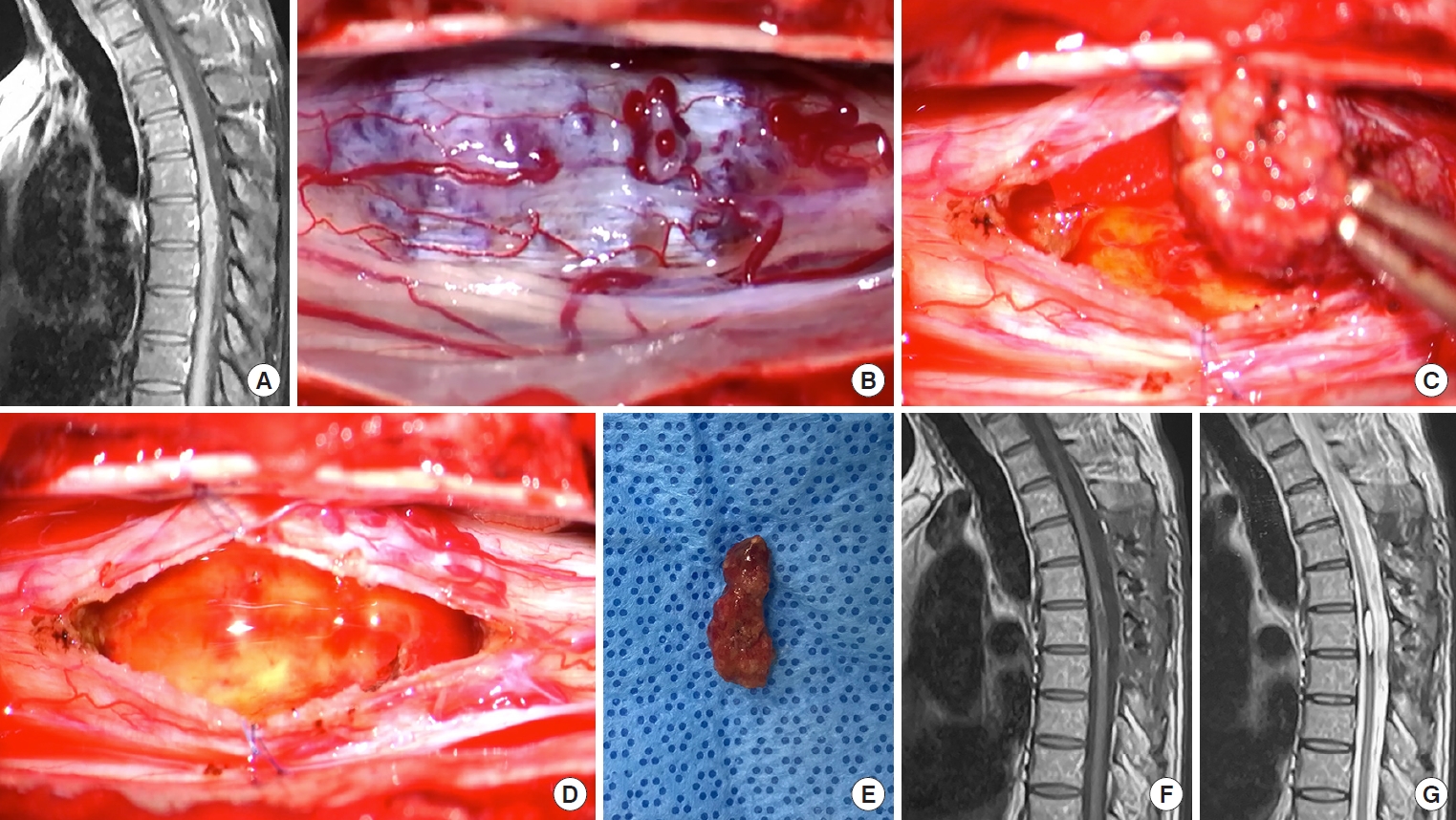
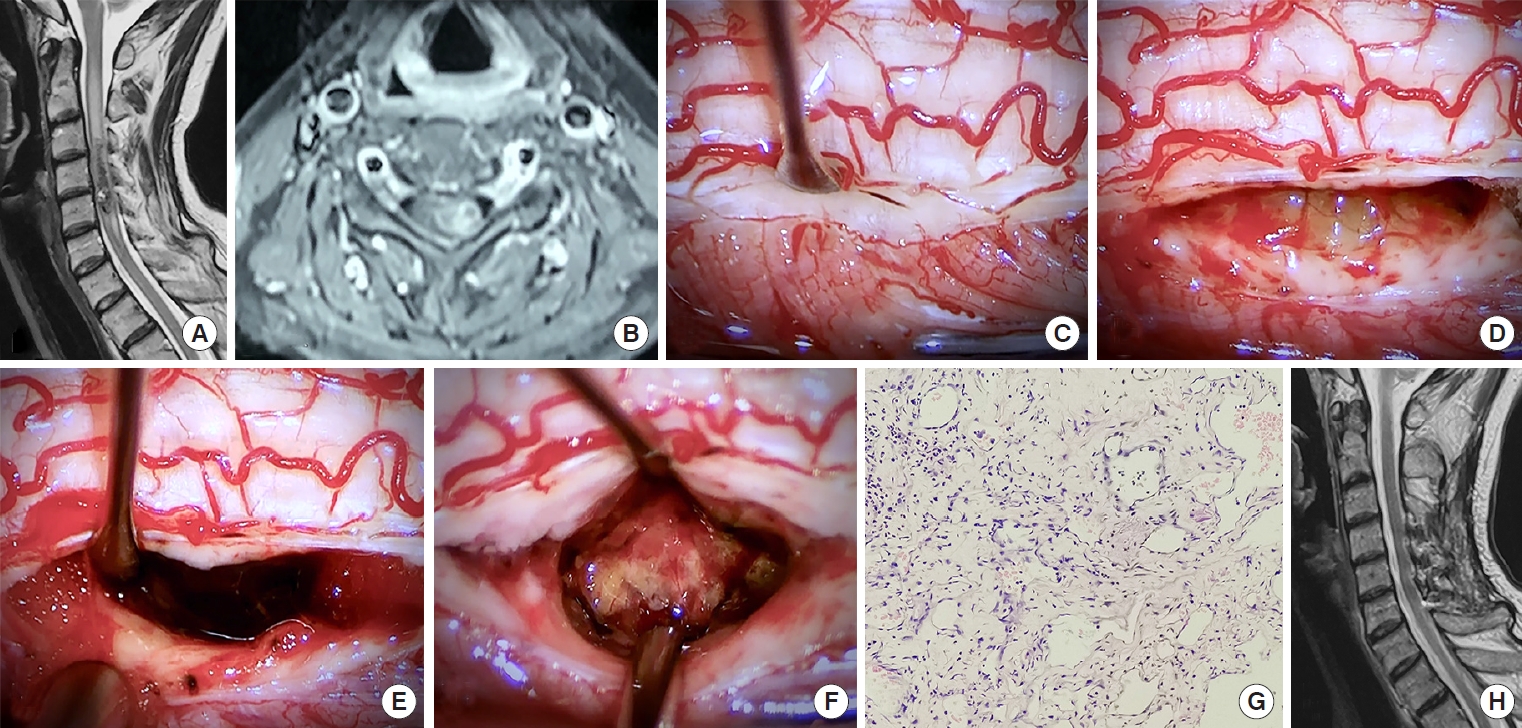
All patients of the present symptomatic ISCMs group received microsurgical treatment mainly by 2 experienced neurosurgeons. Patients were placed in a prone position, with an additional 3-point Mayfield (Codman, Inc., Raynham, MA, USA) or Maquet (MAQUET, Rastatt, Baden-Wuerttemberg, Germany) head holder used for cervical lesions. The conventional posterior approach was used in all the patients via laminectomy or laminoplasty of the appropriate spinal level. One more laminectomy level above or below was performed if the lesion located laterally or ventrally to obtain adequate surgical operation space. The intraoperative monitoring was performed to minimize the risk of injury. After the dura opening was made along the long axis of the thecal sac, a posterior myelotomy was preferably used for lesions in the midline (Fig. 1B–D). A posterolateral sulcus myelotomy, being equivalent to the dorsal root entry zone myelotomy, was used when the lesions were located laterally (Fig. 2C–E). Figs. 1–2 illustrate 2 representative examples of different spinal cord myelotomy approaches. The typical changes associated with the lesion in intraoperative findings were discoloration or hemosiderin deposition, partially accompanied by fresh hemorrhage. The lesion was removed en bloc along the gliotic plane surrounding the malformation.
After resection, the tumor bed was explored carefully to exclude residual vascular malformations, followed by layer-to-layer and water-tight suturing of the dura. All patients were routinely followed at outpatient clinics at 3, 6, and 12 months and subsequently assessed every year by outpatient visits or by telephone. MRI was regularly performed in the first 3 years after discharge, and then every 3 years. The long-term surgical outcome was based on follow-up from the time of surgery to the most recent medical information. The mean follow-up period was 4.8 years (1.6 years to 8.8 years). The outcome data included the patient’s current neurological status compared with their preoperative clinical presentation results.
4. Statistical Analysis
Descriptive statistics were performed to assess baseline patients’ demographic and clinical characteristics. Continuous variables were compared using the Kruskal-Wallis correlation test, while categorical variables were compared using the chisquare test or Fisher exact test. A p-value of < 0.05 signified a statistically significant difference. Statistical analyses were performed using IBM SPSS Statistics ver. 25.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Baseline Characteristics and Clinical Presentation
A total of 29 patients (17 males, 58.6%) met inclusion criteria (Fig. 3). The mean age of the patients was 45.2±14.3 years (range, 17–69 years). The majority of lesions were located in the thoracic spinal cord (n= 15, 51.7%), followed by the cervical (n= 12, 41.4%) and cervicomedullary junction (n= 2, 6.9%). The mean size of the lesions was 9.7 mm (range, 3–20 mm). Most patients suffered a bowel or/and bladder dysfunction symptom (n= 11, 37.9%), followed by sensory deficits (n= 5, 17.2%), gait disturbance (n= 5, 17.2%), pain (n= 4, 13.8%), and weakness (n= 4, 13.8%). Seven patients (24.1%) had severe neurological deficits with grade IV/V on the MMcS. According to the classification of patients’ clinical presentation, 12 cases (41.4%) were classified as type A, 15 cases (51.7%) as type C, and 2 cases (6.9%) as type M. Detailed description of baseline characteristics and clinical presentation were illustrated in Tables 2–3.
2. The Risk Associated With Hemorrhage Events
A total of 27 hemorrhagic episodes were observed in 1,310 patient-years. The calculated annual retrospective hemorrhage rate for symptomatic ISCMs was 2.1% per patient/year. A total of 27 hemorrhages occurred in the 18 patients, with 50.0% (n= 9) of patients experienced rehemorrhage events before the initial clinical visit to our hospital. A significantly higher proportion of patients in the hemorrhage group had smaller lesion size (p= 0.008). In addition, hemorrhage can also be suggested by the patient’s acute onset (p= 0.036) and higher MMcS on presentation (p= 0.003). Thirty-one percent cases (n= 9) had rehemorrhage events before the treatment. No statistically significant differences were found between the 2 groups regarding age, sex, location, symptom types, and duration before the presentation (Table 4).
3. Surgical Outcomes and Prognostic Factors
All patients received total resection of the lesions without subsequent bleeding or rehemorrhages during follow-up. According to the MMcS measured at the last postoperative follow-up, 19 patients improved, 4 patients remained stable, and 6 patients worsen compared with preoperative status. The 6 patients who decline mainly suffered numbness and pain. The patients were divided into improved and not-improved groups according to neurological outcomes. Patient age, sex, tumor size, tumor location, symptom types, symptom duration, clinical course before presentation, preoperative MMcS, and history of hemorrhage were analyzed, respectively with patient outcomes. The 2 groups observed no statistically significant differences in sex, tumor location, tumor size, or symptom type. We found that older patients had better outcomes than younger ones (p= 0.009). Neurological improvement was more frequently seen in patients with a more prolonged course (p= 0.015) and the chronic onset of disease (p = 0.003). We also found that patients with lower preoperative MMcS had better outcomes (p = 0.035). Overall neurological results were not significantly correlated with the initial hemorrhage before surgical treatment (p = 0.530), but those were worse in patients with a history of recurrent hemorrhages (p= 0.016). Detailed statistical data are presented in Table 5.
DISCUSSION
1. Demographics
CMs occur mostly intracranially and rarely in the spinal cord. With the increased availability of MRI, the detection rate of ISCMs has increased. However, the true incidence of ISCMs remains unclear [15]. Jellinger [16] has suggested that ISCMs represent 5%–12% of all spinal vascular diseases. Liang et al. [17] have estimated that the incidence of ISCMs represented 8.7% of spinal vascular diseases. Our calculated incidence of ISCMs is 10.5% of spinal vascular diseases, similar to previously published rates. Appiah et al. [18] included 157 patients for analysis and showed that 51% of the lesions were in the epidural, 34% in the intramedullary, and 15% in the perimedullary. Histologically, they consist of endothelial-lined vascular spaces of varying sizes embedded in a connective tissue matrix, lacking apparent arteries for blood supplement and draining veins. Multiple small vessels can be seen entering the lesion, and there are often small foci of hemorrhage within or around it [18] (Fig. 2G). A female prevalence in the population with ISCMs has been reported, with a female-to-male ratio of approximately 2:1 [19,20]. Interestingly, the ratio in our study was 1:1.4. When it comes to the distribution of lesions in the spinal cord, the cervical and thoracic cord occurred in comparable proportions in this series (48.3% vs. 51.7%). This result is identical to the findings of a large meta-analysis conducted by Badhiwala et al. [4], which included 631 patients. It has also been shown that lesions are more likely to arise in the thoracic. The mean age of onset in this series was 45.2 years (range, 17–69 years), which was concordant with previous literature [17,18]. Most patients in our series tended to present with chronic progressive myelopathy (type C). Chronic progressive symptoms are thought to occur due to microhemorrhage of intralesion, microcirculatory changes, and partial thrombosis [20]. In other patients, there was a rapid deterioration of neurological function (type A) due to acute hemorrhage within the ISCMs.
2. Hemorrhage Events
It is well known that hemorrhage was an essential factor in the progression of patients suffering from ISCMs. The annual hemorrhage rate for the present group of patients was calculated to be approximately 2.1%. This was consistent with the rate of 1.4%–6.8% previously reported in the literature [21,22]. Some researchers have conducted follow-up studies of ISCMs patients in the conservative group and found an annual hemorrhage rate of about 3.9%–5.5%. This figure may better reflect the actual situation [21,23]. Our study showed that the lesions in the thoracic group had a higher risk of hemorrhage than the cervical group. This may be due to the smaller space in the thoracic spinal canal, resulting in a poorer tolerance of the patient. While in the cervical group, the patients ignore some of the older hemorrhagic events that may be smaller and cause less severe symptoms because of recall bias. In addition, we observed a higher incidence of hemorrhage in smaller lesions, which contradicts Tong’s results [8]. However, the study of Goyal et al. [7] did not demonstrate a clear relationship between hemorrhage events and lesion size in ISCMs, but did find a significantly greater risk of hemorrhage in lesions larger than 1 cm. Consequently, larger amounts of case data are needed to elucidate this issue. There was no significant correlation between the initial presence or absence of hemorrhage and the outcomes of the patient; however, it is noteworthy that patients with a history of recurrent hemorrhage had significantly worse results. While a subset of patients may remain neurologically and clinically stable after initial presentation, a small prospective study suggests a very high annual rehemorrhage rate after that [22]. Additionally, several patients in this series experienced acute hemorrhage resulting in a dramatic decline in neurological function that did not return to their prehemorrhagic state even after surgery, so we believe that in cases with a high risk of hemorrhage, such as lesions located in the thoracic spine and history of prior hemorrhage, Surgical treatment should be considered to benefit the patient and avoid subsequent rehemorrhage resulting in severe neurological deficits.
3. Surgical Outcomes
GTR can be accomplished safely and is an available option for the treatment of ISCMs [24]. Although a transient deterioration may occur after surgery, most improved postoperatively after 3 to 6 months. Outcomes of patients were attributed to a variety of factors. In an extensive pooled analysis, Badhiwala et al. [4] found that lesions > 10 mm, duration of disease < 3 months, via hemilaminectomy, and GTR, were factors associated with improved neurological function in patients after surgery. Zhang et al. [25] found that patients with lesions located in the cervical cord had better outcomes because of earlier defect detection and better intraoperative visualization. Our study showed that patient outcomes were not correlated with lesion location and size. Meanwhile, we found that initial hemorrhage was not a risk factor for results, even though the patients may suffer an acute neurological deterioration before surgical treatment. Zhang et al. [22] emphasized the importance of conservative treatment for asymptomatic or less symptomatic patients. This result should be viewed with caution because based on previous literature and the results of this study, satisfactory outcomes can be achieved with surgical treatment of this disease when the surgical strategy is carefully planned. Badhiwala et al. [4] counted a total of 631 patients in 40 publications, and a total of 567 patients were treated surgically, of which 264 (51.5%) improved, 194 (37.8%) remained unchanged, and 55 (10.7%) worsened. For 64 patients in the conservative treatment group, only 16 (30.2%) had improved neurological function, 31 (58.5%) remained unchanged, while 17 (11.3%) experienced a neurological decline. Compared with conservative, resection was significantly associated with favorable neurological outcomes (odds ratio, 2.97; 95% confidence interval, 1.46–5.33; p= 0.002). Therefore, this data should not be overinterpreted as evidence favoring conservative management. Our standard protocol is to perform surgical resections for patients with symptomatic ISCMs, especially those with a history of recurrent hemorrhages.
4. Surgery Timing
As a kind of vascular disease, when the surgical decision is made for symptomatic ISCM patients, the perfect timing of surgical management should also be considered.
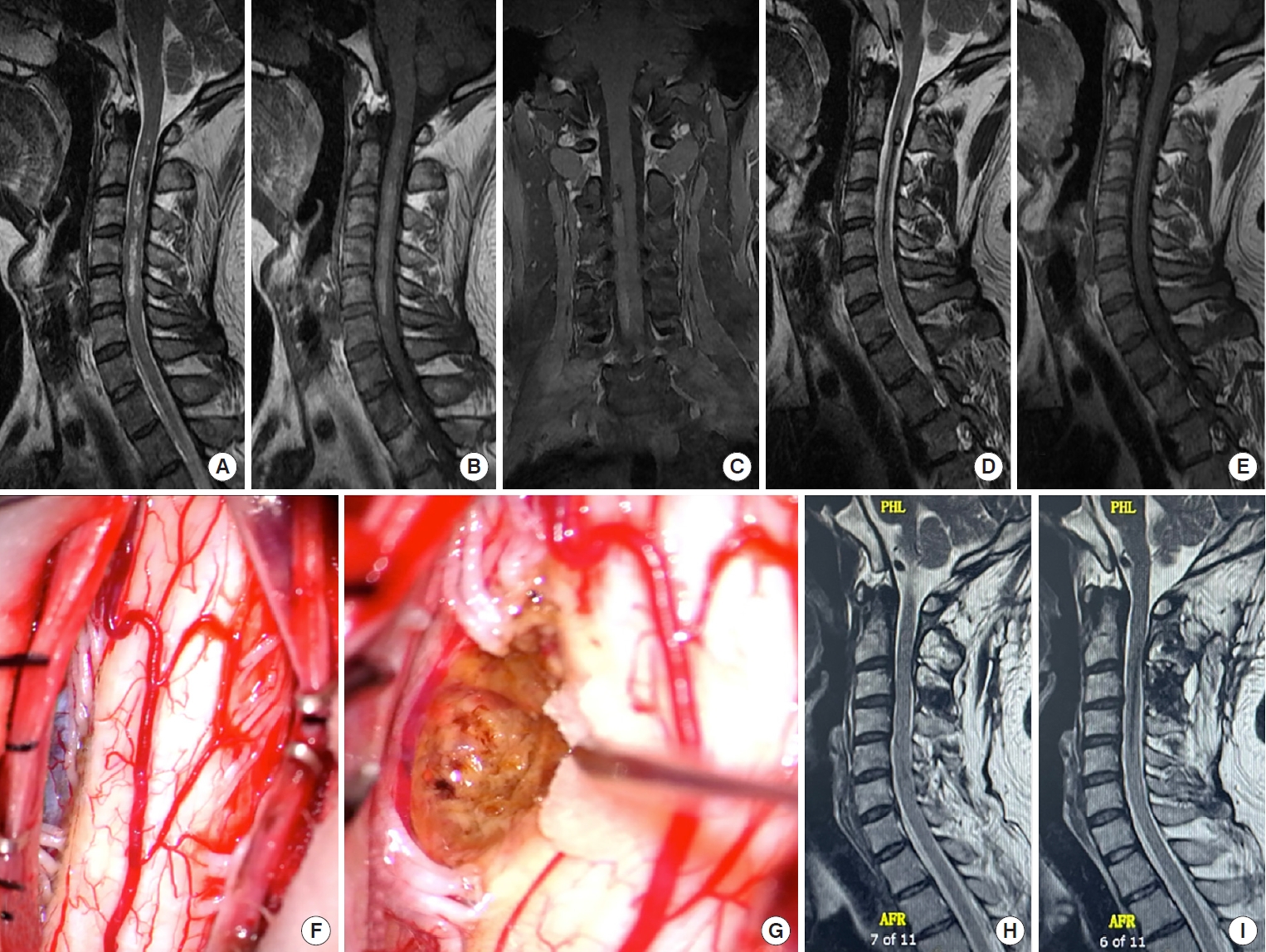
Some authors have argued that early surgical intervention is recommended for a better surgical outcome [4,26]. Other authors, however, hold a different view. Zevgaridis et al. [27] argued that if surgery is to be performed for cavernomas in critical areas, 4± 6 weeks after a hemorrhage seems to be the optimal point in time. A glial scar has developed, and the hematoma is in resolution and can be used to the surgeon’s advantage. Following the decompression of the hematoma, there is sufficient space to excise the malformation. Kondziella et al. [28] also argued that if a decision in favor of surgical excision is made, subacute intervention after 4–6 weeks seems optimal when the hematoma is in resolution and a glial scar develops. Zhang et al. [29] reported 18 cases of pediatric ISCMs treated outcomes. 3 of the patients (16.7%) underwent emergence surgery immediately after hospitalization, and 2 patients (11.1%) underwent surgery 7 days after the recent episodes of hemorrhage, these lesions were found to adhere tightly to the spinal cord without an obvious gliotic plane, and the resection process was technically challenging. Two of them underwent STR since total resection was deemed unsafe. In a patient with an acute hematoma onset, the hemorrhagic stimulation and subsequent extensive edema were often the main causes of neurological deterioration, rather than the lesion itself. For such patients, we also advocate that conservative treatment should be given for 4–6 weeks before surgery, pending the absorption of the hematoma and edema, and that neurological function can generally be largely restored. After most of the hematoma and edema were absorbed, a clear operating boundary was formed, conducive to surgical separation and reducing the risk of secondary injury and residual lesions (Fig. 4).
5. Limitations
Despite the present report focusing on the point of the symptomatic ISCMs with a relatively large number of consecutive cases, the study cohorts are still limited due to the rarity of the lesions. We assessed the data from a single center, which can lead to well-known information and selection biases. More case series with large cohorts are still needed, and a prospective multicenter randomized study or a registry for patients with ISCMs is highly recommended. Despite these limitations, our study still provided comprehensive information on this rare entity to aid treatment strategy-making.